Complications and risk factors of intramedullary bone lengthening nails: a retrospective multicenter cohort study of 314 FITBONE and PRECICE nails
Markus W FROST 1,2, Ole RAHBEK 1,2, Christopher IOBST 3, Anirejuoritse BAFOR 3, Molly DUNCAN 3, and Søren KOLD 1,2
1 Department of Orthopedic Surgery, Aalborg University Hospital; Aalborg; 2 Department of Clinical Medicine, Faculty of Medicine, Aalborg University, Aalborg, Denmark; 3 Department of Orthopaedic Surgery, Center for Limb Lengthening and Reconstruction, Nationwide Children’s Hospital, Columbus, OH, USA
Background and purpose — Intramedullary bone-lengthening nails have become increasingly popular. The 2 most used and successful nails are the FITBONE and the PRECICE nails. Uniform reporting is lacking on complications of intramedullary bone-lengthening nails. The purpose was therefore to assess and categorize the complications of lower limb bone-lengthening nails and investigate risk factors.
Patients and methods — We performed a retrospective review of patients operated on with intramedullary lengthening nails at 2 hospitals. We included only lower limb lengthening with FITBONE and PRECICE nails. Recorded patient data was patient demographics, nail information, and any complication. Complications were graded according to severity and origin classification. Complication risk factors were assessed with modified Poisson regression.
Results — 314 segments in 257 patients were included. The FITBONE nail was predominantly used (75%), and most of the lengthenings were performed in the femur (80%). 53% of the patients had complications. 269 complications were identified in 175 segments (144 patients). Device-related complications were most frequent (0.3 complications/segment), followed by joint complications (0.2 complications/segment). An increased relative risk was found for complications in the tibia compared with the femur and for age groups above 30 years compared with the 10–19 years group.
Conclusion — Complications with intramedullary bonelengthening nails were more frequent than has previously been reported, with 53% of patients sustaining a complication. Future studies need to document the complications meticulously so that the true risk can be established.
Citation: Acta Orthopaedica 2023; 94: 51–59. DOI https://doi.org/10.2340/17453674.2023.8479.
Copyright: © 2023 The Author(s). This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (https://creativecommons.org/licenses/by-nc/4.0/), allowing third parties to copy and redistribute the material in any medium or format and to remix, transform, and build upon the material for non-commercial purposes, provided proper attribution to the original work.
Submitted: 2022-04-12. Accepted: 2022-12-29. Published: 2023-02-17.
Correspondence: markus.frost@rn.dk
Conception/design of work: SK, OR, MWF. Acquisition of data: AB, MD, MWF. Analysis of data: MWF. Interpretation of data: SK, OR, MWF. Drafting the work: MWF. Critical revision: SK, OR, CI. Finalization and submission of the manuscript: SK, MD, AB, CI, OR, MWF.
The authors would like to thank Kirsten Duch for skillful and thorough biostatistics assistance.
Handling co-editors: Ivan Hvid and Jonas Ranstam
Acta thanks Hubert Oostenbroek and Jan Rölfing for help with peer review of this study.
Intramedullary bone-lengthening nails were introduced in an attempt to reduce complications with external fixation and improve patient comfort (1,2). The initial mechanically driven intramedullary bone-lengthening nails had challenges controlling the lengthening rate, which was resolved by the introduction of electrical (FITBONE) or magnetically (PRECICE) driven motorized intramedullary bone-lengthening nails (2-7). So far, comparative studies comparing external fixation with FITBONE or PRECICE lengthening nails are few and with small patient samples (8,9). A systematic review on FITBONE and PRECICE nail complications found that the literature is mostly composed of small studies and with inconsistent complication reporting (10). Analysis of the complications, including risk factors, may improve the treatment and shared decision-making with patients. The aim of the study was to review a consecutive treatment series with the FITBONE and the PRECICE lengthening nails from 2 centers to assess the proportion, severity, and origin of complications. The secondary aim was to investigate potential risk factors of sustaining a complication with these lengthening nails.
Patients and methods
Study design and participants
We performed a retrospective cohort series review, according to STROBE guidelines, of intramedullary bone-lengthening nail patients from 2 hospitals: the Nationwide Children’s Hospital (NCH), Ohio, USA and Aalborg University Hospital (AAUH), Denmark. Patients were included if they had a PRECICE (Nuvasive, San Diego, CA, USA) or FITBONE (Orthofix, Lewisville, TX, USA/Wittenstein Intens, Ingersheim, Germany) bone-lengthening nail and if the bone-lengthening nail had been removed after the end of treatment. Exclusion criteria were bone-transport nails, stump-lengthening nails, compression nails, PRECICE STRYDE, nail insertion or removal at a hospital other than NCH or AAUH, lengthening nails in upper extremities, and extramedullary lengthening. The treatment period was 2017–2020 at NCH and 2005–2021 at AAUH. Some patients had multiple segments lengthened. To avoid correlation bias for patients with multiple segments, a random segment was included in the regression analysis. Thus, in the sub-cohort used for regression analysis, only 1 segment of lengthening per person was included.
Over the years, we have adjusted our clinical practice to the importance of blocking screws to ensure deformity correction or to increase the bone-to-nail stability, especially in the tibia (11–13). Rigid reamers are used with the straight nail designs (14,15). To reduce the surgical impact on the soft tissues and especially the knee joint during retrograde femoral nailing, tube systems are used for both inserting and removing nails (16,17).
Measures of demographic characteristics
Patient charts were reviewed to identify age, sex, clinical preoperative limb length discrepancy (short stature patients were reported as zero), and other surgical procedures at nail insertion. Etiology was classified using the Stricker and Hunt classification with an added category: unknown (10,18) (see Supplementary material). Duration of implantation was defined as days between nail insertion and nail removal. Length of follow-up was defined as days from nail insertion to the last follow-up. Deformity was defined as a lack of cortical alignment on the postoperative radiograph. Nail information was bone (femur/tibia), nail approach, nail type (FITBONE/PRECICE), nail length (mm). End length of bone regenerate (total bone length gained) on radiograph was defined as end minus start length of the telescopic male part (mm).
Outcome measures of complication
The primary outcome of complication severity and origin was identified through a review of patient charts. The severity was classified according to Black et al. (Table 1) (9). By definition, deep vein thrombosis, osteomyelitis, and joint subluxation/luxation were graded as type IIIB complications. The manufacturers state that nail removal is mandatory for both FITBONE and PRECICE nails, and therefore we did not classify scheduled and uneventful nail removal as a complication (19,20).
| Complication severity grade | ||
| Examples of complications | ||
| I | Minimal intervention required; treatment goal still achieved | |
| Temporary joint contracture resolved by physiotherapy. Device stop lengthening due to suboptimal placement of the external transmitter, resolved by repositioning of the external transmitter | ||
| II | Substantial change in treatment plan; treatment goal still achieved | |
| Unplanned return to surgery, such as delayed consolidation requiring additional intervention, or device problem needing revision | ||
| IIIA | Failure to achieve treatment goal, no new pathology or permanent sequelae | |
| Premature consolidation with aborted lengthening, inability to tolerate lengthening, and fracture at fixation site or regenerate bone with shortening | ||
| IIIB | Failure to achieve treatment goal and/or new pathology or permanent sequelae | |
| Joint subluxation, joint dislocation, regenerate fracture with deformity, and deep infection. Thromboembolic complication such as deep vein thrombosis | ||
The type of complication was categorized into origin, representing 8 main groups and 33 subgroups according to Frost et al. and by applying a predefined set of interpretations (10) (see Supplementary material).
Complications were assessed in the period from nail insertion to the last follow-up according to the timing of occurrence in the treatment period, which was divided into 6 time slots (intraoperative, postoperative before distraction, distraction, consolidation, intraoperative nail removal, and after nail removal). A subset of the complications after nail removal has previously been reported but is included to provide the complete complication pattern throughout treatment (21).
Outcome measures of risk factors
Clinical and literature subject-matter knowledge was used to pinpoint measurable variables of interest. As multiple variables were of interest, model construction and variables selection were guided by directed acyclic graphs (DAG) (22). DAGs for each outcome variable were created to ensure the appropriateness of regression analysis (Figure 1, see Appendix). Our DAG models led us to investigate the following possible risk factors for complications: age, bone, increasing bone lengthening, femur approach, deformity correction, etiology, previous bone lengthening, and nail type.
Statistics
Continuous variables were described as median, range, and interquartile range (IQR), or mean and standard deviation (SD) as appropriate according to sample distribution. Categorical variables were described with count and proportions with the Wilson confidence interval (CI). In the full cohort complications were reported as complications per segment (Table 5). In the sub-cohort, complications were dichotomized as complications (yes/no) for regression analysis. The overall proportions of complication were reported according to the sub-cohort (Table 4). As regression analysis, a modified Poisson regression with robust CI was used to calculate the relative risk (RR) of a complication (Table 6) for relevant risk factors (23). Both crude and adjusted regression models were chosen based on DAGs (Figure 1, see Appendix). Missing values were observed only in the variables “Time point at which complication first recognized” and “Length of inserted nail.” Both variables were not included in the risk analysis, and therefore sensitivity analyses were not performed. Covariate estimates of regression analysis can be found in Table 2 (see Appendix). Data analysis was performed with Stata/MP 17.0 (StataCorp, College Station, TX, USA). The significance levels were set to 5%, and estimates were given with 95% CI.
| Factor | All segments | Sub-cohort of segments a |
| Lengthened segments | 314 | 257 |
| AAUH, Denmark b | 279 (87) | 223 (87) |
| NCH, USA c | 35 (13) | 34 (13) |
| Patients | 257 | 257 |
| Patients with multiple segments | 35 (14) | 0 |
| 2 lengthened segments | 24 | |
| 3 lengthened segments | 3 | |
| 4 lengthened segments | 7 | |
| 7 lengthened segments | 1 | |
| Male sex | 165 (53) | 143 (56) |
| Female sex | 149 (47) | 114 (44) |
| Age at nail insertion | ||
| median (IQR) | 19.5 (16.4–29.9) | 19.5 (16.4–33.6) |
| (min–max) | (9.5–76.9) | (9.5–76.9) |
| LLD d etiology | ||
| Congenital | 64 (20) | 61 (24) |
| Acquired/developmental | 143 (46) | 133 (52) |
| Short stature | 69 (22) | 25 (10) |
| Unknown | 38 (12) | 38 (15) |
| Median (IQR) preoperative LLD e | 3.1 (2.5–4) | 3.0 (2.5–4) |
| (min–max) | (1–14) | (1–13) |
| Other procedure at primary surgery | 153 (49) | 127 (49) |
| Duration of implantation, days | ||
| median (IQR) | 410 (336–632) | 393 (329–569) |
| (min–max) | (45–2,372) | (45–2,166) |
| Length of follow-up, days) | ||
| median (IQR) | 646 (478–1,073) | 583 (478–1,073) |
| (min–max) | (176–3,718) | (176–3,718) |
| Previous lengthening f | ||
| None | 248 (79) | 214 (83) |
| Segment | 32 (10) | 24 (9) |
| Limb | 34 (11) | 19 (7) |
| Angle correction in frontal or sagittal plane | 80 (25) | 64 (25) |
| a Sub-cohort of segments used for regression analysis of risk is the unique group that by random selection ensures that every patient was represented by only 1 segment. | ||
| b AAUH: Aalborg University Hospital. | ||
| c NCH: Nationwide Children’s Hospital. | ||
| d LLD: Limb length discrepancy | ||
| e Short stature is not included. | ||
| f in the same patient | ||
| Factor | All segments (n = 314) | Sub-cohort of segments a (n = 257) |
| Bone | ||
| Femur | 251 (80) | 208 (81) |
| Tibia | 63 (20) | 49 (19) |
| Right side | 157 (50) | 130 (51) |
| Nail type | ||
| FITBONE | 234 (75) | 191 (74) |
| PRECICE | 80 (26) | 66 (26) |
| Nail approach | ||
| Antegrade femur | 41 (13) | 37 (14) |
| Retrograde femur | 210 (67) | 171 (67) |
| Antegrade tibia | 56 (18) | 44 (17) |
| Suprapatellar tibia | 7 (2) | 5 (2) |
| Length of inserted nail, mm (n = 303) | ||
| median (IQR) | 245 (225–245) | 245 (225–245) |
| (min–max) | (115–365) | (115–365) |
| a See footnote Table 3. | ||
| Factor | Complications severity grade | ||||
| I | II | IIIA | IIIB | Overall a | |
| Full cohort (257 patients with 314 segments) | |||||
| Absolute number of complications | 86 | 144 | 9 | 30 | 269 |
| Complication (yes/no) per segment (CI) | 0.25 (0.21–0.30) | 0.35 (0.30–0.41) | 0.03 (0.01–0.05) | 0.09 (0.06–0.12) | 0.55 (0.50–0.61) |
| Complication (yes/no) per patient (CI) | 0.26 (0.21–0.32) | 0.35 (0.29–0.41) | 0.04 (0.02–0.07) | 0.11 (0.07–0.15) | 0.56 (0.50–0.62) |
| Sub-cohort (257 patients with 257 segments) | |||||
| Absolute number of complications (CI) | 63 | 113 | 7 | 26 | 209 |
| Complication (yes/no) per patient b | 0.23 (0.18–0.28) | 0.33 (0.28–0.40) | 0.03 (0.01–0.06) | 0.09 (0.06–0.14) | 0.53 (0.47–0.59) |
| a The overall proportion is not necessarily equal to the summation of the complication grading when looking at the dichotomized complication outcome. This is obvious as each person or segment may experience multiple complications, which are graded differently. | |||||
| b For the sub-cohort only 1 segment is included for each patient (for the sub-cohort, the complications per patient are equal to the complications per segment). Thus the complication (yes/no) per patient and segment is exactly the same. | |||||
| Factor | Severity grade and origin of complications | ||||
| I | II | IIIA | IIIB | Sum | |
| Soft tissue | |||||
| Skin | 2 | 2 | |||
| Muscles | 1 | 2 | 3 | ||
| Tendons | 0 | ||||
| Pain | 5 | 5 | |||
| Others | 1 | 1 | |||
| Sum (fraction) | 8 | 2 | 1 | 11 (0.04) | |
| Joint | |||||
| Pain | 12 | 2 | 1 | 15 | |
| Contracture | 19 | 19 | 3 | 10 | 51 |
| Subluxation | 2 | 2 | |||
| Dislocation | 0 | ||||
| Others | 2 | 1 | 1 | 4 | |
| Sum (fraction) | 33 | 20 | 5 | 14 | 72 (0.23) |
| Vascular | |||||
| Vascular damage | 2 | 2 | |||
| Deep vein thrombosis | 1 | 1 | |||
| Hemorrhage/hematoma | 0 | ||||
| Others | 0 | ||||
| Sum (fraction) | 3 | 3 (0.01) | |||
| Bone | |||||
| Premature consolidation | 1 | 2 | 3 | ||
| Delayed healing | 2 | 14 | 16 | ||
| Secondary malalignment | 1 | 1 | 1 | 3 | |
| Fracture | 4 | 10 | 14 | ||
| Others | 1 | 1 | |||
| Sum (fraction) | 7 | 27 | 1 | 2 | 37 (0.12) |
| Neurology | |||||
| Paresthesia | 1 | 1 | |||
| Paralysis | 2 | 2 | |||
| Others | 2 | 2 | 4 | ||
| Sum (fraction) | 3 | 4 | 7 (0.02) | ||
| Infection | |||||
| Superficial soft tissue | 2 | 4 | 6 | ||
| Deep soft tissue | 3 | 1 | 4 | ||
| Osteomyelitis | 3 | 3 | |||
| Others | 3 | 1 | 4 | ||
| Sum (fraction) | 5 | 8 | 4 | 17 (0.05) | |
| Device-related | |||||
| Distraction mechanism | 17 | 5 | 22 | ||
| Mechanical strength | 2 | 4 | 1 | 7 | |
| Attachment failure | 1 | 27 | 1 | 29 | |
| Others | 7 | 35 | 42 | ||
| Sum (fraction) | 27 | 71 | 2 | 100 (0.32) | |
| Others | |||||
| Patient | 1 | 1 | 2 | ||
| Surgical | 2 | 14 | 1 | 17 | |
| Others | 1 | 1 | 1 | 3 | |
| Sum (fraction) | 3 | 16 | 1 | 2 | 22 (0.07) |
Ethics, registration, funding, and disclosures
Institutional ethics approval was granted at Nationwide Children’s Hospital (STUDY00000908) and Aalborg University Hospital [project ID. no. 2020-157]). No external funding was received. CI is a consultant for Orthofix, which distributes the FITBONE nail, Wishbone Medical, Inc., Smith & Nephew, and NuVasive, which manufactures the PRECICE nail. AB is a consultant for Wishbone Medical, Inc. SK is a consultant for Wishbone Medical, Inc. The other authors have no conflicts of interest to declare. Completed disclosure forms for this article following the ICMJE template are available on the article page, doi: 10.2340/17453674.2023.8479
Results
Demographic characteristics
We identified 393 consecutive segments lengthened with FITBONE or PRECICE nails, of which 79 segments were excluded (4 segments were lost to follow-up and 75 segments discounted due to the exclusion criteria) (Figure 2). The remaining 314 included segments belonged to 257 patients with a median age of 19.5 years. Demographic data is summarized in Table 3. Most lengthenings were performed in the femur (80% of 314 segments), and the FITBONE nail was used predominantly (75% of 314 segments). Nail demography is presented in Table 4.
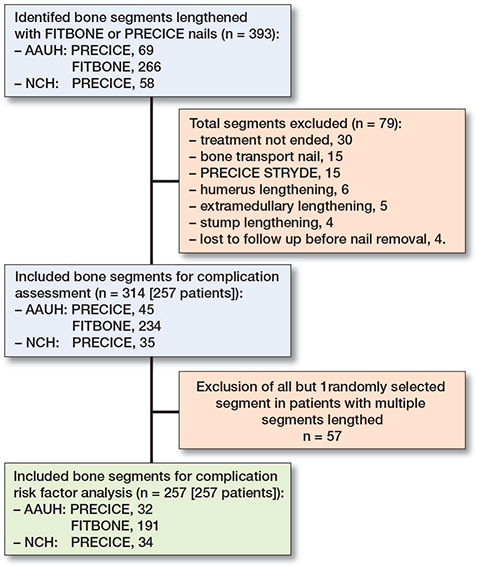
Figure 2. Segment selection flow chart. NCH: Nationwide Children’s Hospital. AAUH: Aalborg University Hospital
Complications
269 complications were identified consisting of 314 (56%) segments (257 patients) and occurred in 175 segments (144 [56%] patients). The proportion of complications per patient was 0.53 (CI 0.47–0.59) in the sub-cohort. The complication distribution on severity grading in the full cohort is presented in Table 5. The median number of complications per segment in the full cohort was 1, with a maximum of 5 complications per segment. Type II complication was the most common complication seen in the proportion 0.35 (CI 0.30–0.41) of patients followed by type I complication seen in 0.25 (CI 0.21–0.31) of patients. Failure to achieve the lengthening goal (type IIIA complication) represented the proportion of 0.03 (CI 0.01–0.05) of patients. A permanent sequela or a new pathology (type IIIB complication) was observed in the proportion of 0.09 (CI 0.06–0.12) of patients.
Device-related complication (Table 6) was the most frequent origin of complications, occurring in 32% of the lengthened segments, but did not result in any type IIIA or IIIB complications. Contracture was the leading cause of joint complications, and the joint was the 2nd most frequent origin of complications as it occurred in 23% of the segments. Bone was the 3rd most frequent origin of complications with complications occurring in 10% of segments.
Of the 268 complications (1 missing data), most occurred during the distraction phase (46% [n = 123]), followed by the consolidation phase (31% [n = 83]), after implant removal (15% [n = 40]), during intraoperative nail removal (3.7% [n = 10]), postoperatively before distraction (2.6% [n = 7]), and intraoperatively (1.9% [n = 5]).
Risk factor analysis (Table 7)
All age groups showed a clinically relevant increased risk of complication in comparison with the reference age group of 10–19 years (both adjusted and crude); however, the age group 20–29 years showed no clinically significantly increased risk compared with the reference. After the age of 30 years the adjusted analysis showed a significant increase in risk of complications with approximately a doubled risk (RR ranged from 1.9 to 2.6) of complication compared with the baseline group. For the age group 20–29 years compared with the older age groups, the largest reduction (40%) was seen when compared with age groups above 50 years. Overall, most age groups showed a statistically significant and a clinically relevant increased risk of complications with increasing age. The etiology short stature as a risk factor showed an 80% complication increase (RR 1.8 [CI 1.2–2.8]) relative to unknown etiology. The estimate of congenital and acquired/developmental etiology showed RR 1.1 (0.7–1.7) and 1.3 (0.90–2.0) complication risk, respectively. The crude model of nail type effect on complication showed a significant 30% risk reduction of the PRECICE nail compared with the FITBONE nail, which was not present in the adjusted model (RR 0.9 [CI 0.7–1.3]). The tibia showed a 70% increased risk of complication (RR 1.7 [CI 1.4–2.0]) compared with the femur, with an estimated effect ranging from 40–100% increased risk, which is interpreted as a clinically important result (Table 7). For bone site, the complication per segment is higher for type I and II complications in the tibia compared with the femur but equal for type IIIA/IIIB (Table 8). The risk of complications was similar between an antegrade or a retrograde approach to the femur (adjusted RR 1 [CI 0.7–1.5]). Previous bone lengthening showed a 10% increase in risk estimate for complication compared with no previous intervention (RR 1.1 [0.8–1.6]). Acute deformity correction presents a 20% higher risk of complications compared with no deformity correction (adjusted RR 1.2 [CI 0.96–1.5]), which would be a clinically significant result but statistically not so. Type I and II complications occurred more often in acute correction osteotomies, but there was no difference for type III complications (Table 8). We found that the risk of complications increased by 1% (RR 1.01 [CI 1.00–1.02]) for every mm lengthened, which is clinically interesting as most patients are lengthened by a minimum of 20 mm, starting with a 20% risk of complication. However, the total effect calculated by adjustment provides no evidence that lengthening increases the risk of complications.
| Factor | Crude model RR (SE) [CI] | Adjusted model (total effect) a RR (SE) [CI] |
| Age (n = 257) | ||
| 10–19 | 1 (reference) | 1 (reference) |
| 20–29 b | 1.6 (0.3) [1.2–2.2] | 1.4 (0.3) [1.0–2.0] |
| 30–39 | 1.9 (0.3) [1.3–2.7] | 2.1 (0.4) [1.4–3.0] |
| 40–49 | 1.8 (0.4) [1.2–2.7] | 1.9 (0.4) [1.3–2.9] |
| 50–59 b | 2.4 (0.4) [1.8–3.3] | 2.6 (0.5) [1.9–3.6] |
| ≥ 60 b | 2.1 (0.4) [1.4–3.1] | 2.3 (0.5) [1.5–3.5] |
| Nail type (n = 257) | ||
| FITBONE | 1 (reference) | 1 (reference) |
| PRECICE | 0.7 (0.1) [0.5–0.9] | 0.9 (0.1) [0.7–1.3] |
| Etiology (n = 257) | ||
| Unknown | 1 (reference) | |
| Congenital | 1.1 (0.3) [0.7–1.7] | |
| Acquired/ developmental | 1.3 (0.3) [0.9–2.0] | |
| Short stature | 1.8 (0.4) [1.2–2.8] | |
| Bone (n = 257) | ||
| Femur | 1 (reference) | 1 (reference) |
| Tibia | 1.7 (0.2) [1.4–2.1] | 1.7 (0.2) [1.4–2.0] |
| Primary osteotomy correction (n = 257) | ||
| No correction | 1 (reference) | 1 (reference |
| Correction | 1.3 (0.2) [1.0–1.6] | 1.2 (0.1) [0.96–1.5] |
| Femur nail approach (n = 208): | ||
| Antegrade | 1 (reference) | 1 (reference) |
| Retrograde | 1.3 (0.3) [0.8–2.0] | 1 (0.2) [0.7–1.5] |
| Previously bone lengthening (n = 257) | ||
| No lengthening | 1 (reference) | 1 (reference) |
| Per leg | 1.2 (0.2) [0.8–1.8] | 1.1 (0.2) [0.7–1.6] |
| Per bone | 1.1 (0.2) [0.8–1.6] | 1.1 (0.2) [0.8–1.6] |
| Total bone length gained (n = 254) | ||
| Length gained per mm | 1.01 (0.004) | 1.01 (0.004) |
| [CI] | [1.0–1.02] | [0.99–1.01] |
| SE: Standard error. | ||
| Sub-cohort of segments used is the group that by random selection ensures that every patient was represented by only 1 segment. Age was grouped into decades from 10 to 60, and > 60 when considering age as a risk factor. When adjusting for age, age was considered continuously to increase power. Dependent variable: complication yes or no for each included observation. | ||
| a In the adjusted model, Age and Bone were adjusted for etiology, Nail type was adjusted for age (continuously variable), bone, and hospital, Previous bone lengthening and Total bone length gained were adjusted for etiology and age (continuously variable), and Primary osteotomy correction and Femur nail approach were adjusted for hospital, etiology, and age (continuously variable). | ||
| b The 20–29 group had a reduction in RR of complication compared with the older age 30–39 (RR 0.7 [CI 0.5–1.0]), 40–49 (RR 0.8 [CI 0.5–1.2]), 50–59 (RR 0.6 [CI 0.4–0.8]), and ≥ 60 (RR 0.6 [CI 0.4–0.96]). | ||
| Factor | Segments | Complications severity grade | Sum | Complication per segment | |||
| n | I | II | IIIA | IIIB | |||
| Nail type | |||||||
| FITBONE | 234 | 72 (0.3) | 121 (0.5) | 7 (0.03) | 24 (0.1) | 224 | 1 |
| PRECICE | 80 | 14 (0.2) | 23 (0.3) | 2 (0.03) | 6 (0.08) | 45 | 0.6 |
| Bone | |||||||
| Tibia | 63 | 25 (0.4) | 54 (0.9) | 1 (0.02) | 7 (0.1) | 87 | 1.4 |
| Femur | 251 | 61 (0.2) | 90 (0.4) | 8 (0.03) | 23 (0.1) | 182 | 0.7 |
| Osteotomy correction | |||||||
| Yes a | 80 | 44 (0.6) | 78 (1) | 7 (0.1) | 21 (0.3) | 150 | 2 |
| No | 234 | 42 (0.2) | 66 (0.3) | 2 (0.01) | 9 (0.04) | 119 | 0.5 |
| a Correction is in frontal or sagittal plane. | |||||||
Discussion
This consecutive series of 314 internal lengthening nails represents to our knowledge the largest cohort to date in examining complications of the FITBONE and PRECICE nails. The main finding was that 53% of the patients had 1 or more complications, which is higher than previously reported (10). Device-related complication was the leading cause of complications. The study by Frommer et al. found complications in 76% of the 90 patients with PRECICE femur lengthening, which is in accordance with our findings (24).
The joint was the 2nd most frequent origin of complications (23% of segments) with contracture as the most prevalent (16% of segments) joint complication. This is in line with temporary joint contractures of 20% reported by Frommer et al. and of 46% reported by Calder et al. (24,25). Joint complications are still an important complication even when the soft-tissue-tethering effect from external fixation has been eliminated. Muscle group imbalance was advocated by Paley as a reason for joint problems in bone lengthening (26).
Age had a high influence on complications with an approximately double risk of complications in the age groups above 30 years. Frommer et al. reported that age above 16 years did not increase the risk of unplanned surgery, but this finding might be due to the low median age (15 years) and small spread of age (14 to 17 years) in their study (24). Zak et al. did not find a risk of advanced age (above 45 years) on bone healing or complication rate when performing bone lengthening with the PRECICE nail; however, the study population was limited to 19 patients (27). The limitations of Frommer et al. and Zak et al. offer a plausible explanation for the differences between their and our results, as our study has larger cohort size, wider age spread, and model substantiated estimate.
Acute deformity correction followed by gradual limb lengthening has been reported to increase complication rates ranging from 15% to 45% (11,28,29). In our model, acute deformity correction showed an RR of 1.2 (CI 0.96–1.5) and we can therefore neither confirm nor reject the findings, even though the point estimate supports the 3 studies.
The tibia showed a 70% increased risk of complication compared with the femur, which is supported by 3 studies on bone-lengthening nails that disclose an increased complication risk of 50–82% (24,30,31).
In the crude model, the risk of total bone length gained showed a significant estimate of 1% increased risk per mm, which was insignificant in the adjusted model. This model of total bone length gained is a pendant to earlier models of increased risk of complication associated with the relative bone lengthening that has been shown for both children and adults (32,33).
Our study is subject to the limitations of the observational nature and retrospective design, which could lead to underreporting, lack of precision in reporting, and only demonstrating associations and not showing causality (34). A retrospective assessment of complications is, however, needed to perform the complication severity grading (9,35). The use of a severity grading standardizes our results, making them easier to assess and compare with others. When comparing our results, it became evident that the area of complication is lacking the gold standard for reporting complications. We have encountered 4 different severity gradings (Paley, Black et al., Dahl et al., Dinçyürek et al.) in studies on bone lengthening nails but many use a descriptive approach and some without defining complications (9,26,36-39). The comparison of complication rates between studies is compromised due to the lack of uniform reporting.
We partly accommodated the risk of observer bias by assigning a researcher not involved in the patient treatment to perform the patient chart evaluation and complication grading. However, bias might have occurred due to imprecise reporting of the complications in the patients’ charts. Bias could also be introduced because the treating physicians participated in the data interpretation. The dominant risk of bias for this study is selection bias, as bone lengthening with external fixators was applied to the most severe cases treated in the same period. These biases would tend to underestimate the true incidence of complications with intramedullary bone-lengthening nails. Only 1% (4/318) of segments were lost to follow-up, which reduces the risk of transfer bias. The lack of interobserver reliability assessment of the applied complication classifications system is a study weakness. However, the complication classification system was tested with an excellent result by 2 raters as reported by Frost et al. (10,40). At AAUH, multiple surgeons have been involved in the treatment for a long period as opposed to NCH, where the same surgeon treated all patients. FITBONE nails and tibial lengthening were performed only at AAUH.
Conclusion
This study showed complications in 53% of patients lengthened with intramedullary bone-lengthening nails. Device-related complications were most frequently seen with 0.3 complications per segment, followed by joint complications with 0.2 complications per segment. There was a higher relative risk for complications in the tibia compared with the femur and age groups above 30.
Supplementary material
Tables showing Disease etiology (18) and Complication origin (10) are available in the Supplementary material file on the article page, doi: 10.2340/17453674.2023.8479
- Hankemeier S, Pape H C, Gosling T, Hufner T, Richter M, Krettek C. Improved comfort in lower limb lengthening with the intramedullary skeletal kinetic distractor: principles and preliminary clinical experiences. Arch Orthop Trauma Surg 2004; 124(2): 129-33. doi: 10.1007/s00402-003-0625-6.
- Simpson A H W R, Shalaby H, Keenan G. Femoral lengthening with the Intramedullary Skeletal Kinetic Distractor. J Bone Joint Surg Br 2009; 91-B(7): 955-61. doi: 10.1302/0301-620X.91B7.21466.
- Guichet J-M, Deromedis B, Donnan L T, Peretti G, Lascombes P, Bado F. Gradual femoral lengthening with the Albizzia intramedullary nail. J Bone Joint Surg Am 2003; 85(5): 838-48. doi: 10.2106/00004623-200305000-00011.
- Baumgart R, Betz A, Schweiberer L. A fully implantable motorized intramedullary nail for limb lengthening and bone transport. Clin Orthop Relat Res 1997; 343(343): 135-43. PMID: 9345218.
- Shabtai L, Specht S C, Standard S C, Herzenberg J E. Internal lengthening device for congenital femoral deficiency and fibular hemimelia. Clin Orthop Relat Res 2014; 472(12): 3860-8. doi: 10.1007/s11999-014-3572-3.
- Paley D, Harris M, Debiparshad K, Prince D. Limb lengthening by implantable limb lengthening devices. Tech Orthop 2014; 29(2): 72-85. doi: 10.1097/BTO.0000000000000072.
- Kirane Y M, Fragomen A T, Rozbruch S R. Precision of the PRECICE® Internal Bone Lengthening Nail. Clin Orthop Relat Res 2014; 472(12): 3869-78. doi: 10.1007/s11999-014-3575-0.
- Horn J, Grimsrud Ø, Dagsgard A H, Huhnstock S, Steen H. Femoral lengthening with a motorized intramedullary nail: a matched-pair comparison with external ring fixator lengthening in 30 cases. Acta Orthop 2015; 86(2): 248-56. doi: 10.3109/17453674.2014.960647.
- Black S R, Kwon M S, Cherkashin A M, Samchukov M L, Birch J G, Jo C-H. Lengthening in congenital femoral deficiency. J Bone Joint Surg Am 2015; 97(17): 1432-40. doi: 10.2106/JBJS.N.00932.
- Frost M W, Rahbek O, Traerup J, Ceccotti A A, Kold S. Systematic review of complications with externally controlled motorized intramedullary bone lengthening nails (FITBONE and PRECICE) in 983 segments. Acta Orthop 2021; 92(1): 120-7. doi: 10.1080/17453674.2020.1835321.
- Iobst C A, Rozbruch S R, Nelson S, Fragomen A. Simultaneous acute femoral deformity correction and gradual limb lengthening using a retrograde femoral nail. J Am Acad Orthop Surg 2018; 26(7): 241-50. doi: 10.5435/JAAOS-D-16-00573.
- Muthusamy S, Rozbruch S R, Fragomen A T. The use of blocking screws with internal lengthening nail and reverse rule of thumb for blocking screws in limb lengthening and deformity correction surgery. Strateg Trauma Limb Reconstr 2016; 11(3): 199-205. doi: 10.1007/s11751-016-0265-3.
- Fürmetz J, Bösl S, Schilling J, Wolf F, Degen N, Thaller P H. Blocking screws for alignment control in intramedullary limb lengthening. Injury 2017; 48(7): 1597-1602. doi: 10.1016/j.injury.2017.03.043.
- Fragomen A T, Rozbruch S R. Lengthening and deformity correction about the knee using a magnetic internal lengthening nail. SICOT J 2017; 3: 25. doi: 10.1051/sicotj/2017014.
- Kucukkaya M, Karakoyun Ö, Erol M F. The importance of reaming the posterior femoral cortex before inserting lengthening nails and calculation of the amount of reaming. J Orthop Surg Res 2016; 11(1): 1-8. doi:10.1186/s13018-016-0345-6.
- Rölfing J D, Bünger M, Petruskevicius J, Abood A A. Removal of broken PRECICE Stryde intramedullary lengthening nails. Orthop Traumatol Surg Res 2021; 107(8): 1-4. doi: 10.1016/j.otsr.2021.102958.
- Iobst C, Kold S, Mikuzis M. Removal of femoral lengthening nails. J Pediatr Orthop Soc North Am 2022; 4(2): 1-18. doi: 10.55275/JPOSNA-2022-0031.
- Stricker S J, Hunt T. Evaluation of leg length discrepancy in children. Int Pediatr 2004; 19(3): 134-46.
- WITTENSTEIN intens. Nail mManual: FITBONE® TAA surgical technique for tibia/femur. Doc-Nr. 6091-D001185. Igersheim, Germany; 2009.
- NuVasive. Nail Manual: antegrade and retrograde femur operative technique. 16-NUVA-0740. San Diego, CA.
- Frost M W, Kold S, Rahbek O, Bafor, Duncan A M, Iobst C A. Complications in elective removal of 271 bone lengthening nails (FITBONE, PRECICE and STRYDE). Strateg Trauma Limb Reconstr 2021; 16(2): 110-5. doi: 10.5005/jp-journals-10080-1529.
- Shrier I, Platt R W. Reducing bias through directed acyclic graphs. BMC Med Res Methodol 2008; 8(70): 1-15. doi:10.1186/1471-2288-8-70.
- Chen W, Qian L, Shi J, Franklin M. Comparing performance between log-binomial and robust Poisson regression models for estimating risk ratios under model misspecification. BMC Med Res Methodol 2018;18(1): 63. doi: 10.1186/s12874-018-0519-5.
- Frommer A, Roedl R, Gosheger G, Niemann M, Turkowski D, Toporowski G, et al. What are the potential benefits and risks of using magnetically driven antegrade intramedullary lengthening nails for femoral lengthening to treat leg length discrepancy? Clin Orthop Relat Res 2022; 480(4): 790-803. doi: 10.1097/CORR.0000000000002036.
- Calder P R, McKay J E, Timms A J, Roskrow T, Fugazzotto S, Edel P, et al. Femoral lengthening using the Precice intramedullary limb-lengthening system. Bone Joint J 2019; 101-B(9): 1168-76. doi: 10.1302/0301-620X.101B9.BJJ-2018-1271.R1.
- Paley D. Problems, obstacles, and complications of limb lengthening by the Ilizarov technique. Clin Orthop Relat Res 1990; 250: 81-104. PMID: 2403498.
- Zak L, Arnhold R, Tiefenboeck T M, Wozasek G E. The influence of advanced age in bone healing after intramedullary limb lengthening. Orthop Traumatol Surg Res 2021; 107(8): 103055. doi: 10.1016/j.otsr.2021.103055.
- Horn J, Hvid I, Huhnstock S, Breen A B, Steen H. Limb lengthening and deformity correction with externally controlled motorized intramedullary nails: evaluation of 50 consecutive lengthenings. Acta Orthop 2019; 90(1): 81-87. doi: 10.1080/17453674.2018.1534321.
- Hammouda A, Szymczuk V, Gesheff M, Mohamed N S, Conway J D, Standard S, et al. Acute deformity correction and lengthening using the PRECICE magnetic intramedullary lengthening nail. J Limb Lengthening Reconstr 2020; 6(1): 20. doi: 10.4103/jllr.jllr_6_20.
- Radler C, Mindler G T, Stauffer A, Weiß C, Ganger R. Limb lengthening with Precice Intramedullary Lengthening Nails in children and adolescents. J Pediatr Orthop 2021 ;42(2): e192-e200. doi: 10.1097/BPO.0000000000002016.
- Wright S E, Goodier W D, Calder P. Regenerate deformity with the precice tibial nail. Strateg Trauma Limb Reconstr 2020; 15(2): 98-105. doi: 10.5005/jp-journals-10080-1457.
- Oostenbroek H J, Brand R, Van Roermund P M. Lower limb deformity due to failed trauma treatment corrected with the Ilizarov technique: factors affecting the complication rate in 52 patients. Acta Orthop 2009; 80(4): 435-9. doi: 10.3109/17453670903153535.
- Antoci V, Ono C M, Antoci V Jr, Raney E M. Bone lengthening in children: How to predict the complications rate and complexity? J Pediatr Orthop 2006; 26(5): 634-40. doi: 10.1097/01.bpo.0000229977.31931.69.
- Martin R C G, Brennan M F, Jaques D P. Quality of complication reporting in the surgical literature. Ann Surg 2002; 235(6): 803-13. doi: 10.1097/00000658-200206000-00007.
- Cherkashin A M, Samchukov M L, Birch J G, Da Cunha A L M. Evaluation of complications of treatment of severe Blount’s disease by circular external fixation using a novel classification scheme. J Pediatr Orthop B 2015; 24(2): 123-30. doi: 10.1097/BPB.0000000000000138.
- Dahl M T, Gulli B, Berg T. Complications of limb lengthening: a learning curve. Clin Orthop Relat Res 1994; (301): 10-18.
- Wiebking U, Liodakis E, Kenawey M, Krettek C. Limb lengthening using the PRECICETM Nail system: complications and results. Arch Trauma Res 2016; 5(4): e36273. doi: 10.5812/atr.36273.
- Tillotson L O, Maddock C L, Hanley J, Arseneau G M, Bradley C S, Kelley S P. Femoral lengthening in children: a comparison of motorized intramedullary nailing versus external fixation techniques. J Pediatr Orthop 2022; 42(5): 253-9. doi: 10.1097/BPO.0000000000002120.
- Dinçyürek H, Kocaoǧlu M, Eralp I L, Bilen F E, Dikmen G, Eren I. Functional results of lower extremity lengthening by motorized intramedullary nails. Acta Orthop Traumatol Turc 2012; 46(1): 42-9. doi: 10.3944/aott.2012.2671
- Svanholm H, Starklint H, Gundersen H J, Fabricius J, Barlebo H, Olsen S. Reproducibility of histomorphologic diagnoses with special reference to the kappa statistic. APMIS 1989; 97(7-12): 689-98. doi: 10.1111/j.1699-0463.1989.tb00464.x.
Appendix
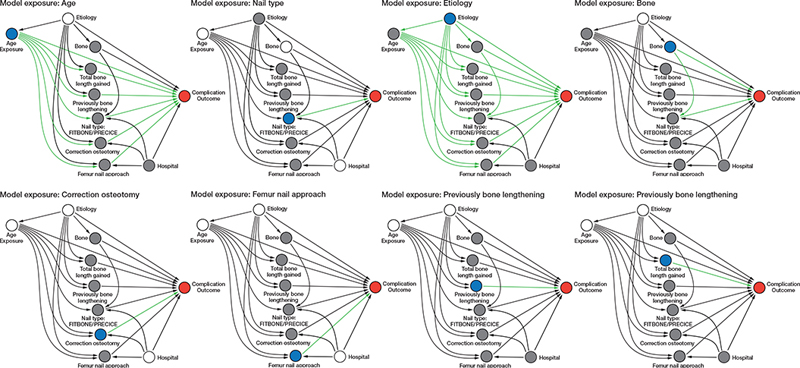
Figure 1. The 8 directed acyclic graphs (DAG) of models used for risk assessment of complication. ●: Exposure. ●: Outcome. ●: Covariates with unknown value/not included in the model. ○ Covariates use to reduce bias. ➞ represent the total effect described by the DAC model.