Smoking is associated with an increased risk of fractures in women: a nationwide population-based cohort study in Finland
Matias VAAJALA 1, Ilari KUITUNEN 2,3, Lauri NYRHI 1,4, Ville PONKILAINEN 4, Tuomas T HUTTUNEN 1,5, and Ville M MATTILA 1,6
1 Faculty of Medicine and Life Sciences, University of Tampere, Tampere; 2 Department of Pediatrics, Mikkeli Central Hospital, Mikkeli; 3 Institute of Clinical Medicine and Department of Pediatrics, University of Eastern Finland, Kuopio; 4 Department of Surgery, Central Finland Central Hospital Nova, Jyväskylä; 5 Department of Anesthesia and Intensive Care, Tampere Heart Hospital, Tampere University Hospital, Tampere; 6 Department of Orthopaedics and Traumatology, Tampere University Hospital, Tampere, Finland
Background and purpose — Smoking weakens bone health and increases the risk of fractures. We investigated the incidence of fractures in smoking, fertile-aged women and compared it with that of non-smoking, fertile-aged women using data from nationwide registers.
Patients and methods — We conducted a retrospective register-based nationwide cohort study from 1998 to 2018. We identified all women smoking during pregnancy from the Medical Birth Register and compared these with non-smokers. We gathered fractures for both groups from the Care Register for Health Care. Pregnancies with missing smoking or socioeconomic status were excluded. A Cox regression model was used to analyze adjusted hazard ratios (aHR) with 95% confidence intervals (CI) for fractures during the 5-year follow-up starting from delivery. The model was adjusted for the age of the mother at the time of delivery and socioeconomic status.
Results — The smoking group included 110,675 pregnancies and the non-smoking group 628,085 pregnancies. The overall fracture rate was higher in smokers after 1-year follow-up (aHR 1.7, CI 1.5–2.0) and 5-year follow-up (aHR 1.7, CI 1.6–1.8). After 5-year follow-up, the fracture rates for polytraumas (aHR 2.3, CI 1.4–3.7), inpatient admitted fractures (aHR 2.0, CI 1.7–2.4), and non-admitted fractures (aHR 1.8, CI 1.7–1.9) were all higher among smoking women.
Conclusion — Smoking in fertile-aged women was associated with a higher risk of fractures during the 1-year and 5-year follow-up after giving birth, also after adjusting for age and socioeconomic status. Whether the increased fracture risk is caused by direct effects of smoking on bone health or riskier behavior remains uncertain.
Citation: Acta Orthopaedica 2022; 93: 859–865. DOI http://dx.doi.org/10.2340/17453674.2022.5275.
Copyright: © 2022 The Author(s). This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (https://creativecommons.org/licenses/by-nc/4.0/), allowing third parties to copy and redistribute the material in any medium or format and to remix, transform, and build upon the material for non-commercial purposes, provided proper attribution to the original work.
Submitted: 2022-06-30. Accepted: 2022-11-02. Published: 2022-11-25.
Correspondence: Matias.vaajala@tuni.fi
MV wrote the initial manuscript. IK and VM undertook the study design. VM supervised the study. VP, TH, and LN helped planning appropriate statistical analysis. Each author commented on the manuscript during the process and confirmed the final version to be submitted.
Handling co-editors: Bart Swierstra and Robin Christensen
Acta thanks Mette Rasmussen for help with peer review of this study.
Smoking is one of the biggest health problems worldwide, contributing to approximately 5 million deaths each year (1). According to a recent systematic review, the current global prevalence of smoking in the general population by women is estimated to be around 17% (2). The pooled prevalence of women ever smoking was highest, 38%, in Europe (2). In Finland the rate of smokers has decreased during last 2 decades in adults from 19% (2000) to 13% (2018) (3). According to the Finnish Institute for Health and Welfare, the less educated smoke more than those with a higher education in Finland (4).
Smoking is known to be associated with numerous health problems, such as respiratory and cardiovascular disorders, cancers, and disorders in bone metabolism (5-7). Smoking is known to cause an imbalance in bone turnover, making smokers prone to lower bone mass and osteoporosis, putting them at a higher risk of fractures (7). In addition to an increased risk of fractures, smokers experience more complications with delayed bone healing, even if they have already stopped smoking, because some adverse effects persist for a prolonged period (8). Females, especially after menopause, are at higher risk of osteoporosis than males (9). However, women of premenopausal age are also known to have an increased risk of osteoporosis. Unhealthy lifestyle (e.g., nutritional deficiency, lack of exercise, high BMI, and use of alcohol or tobacco) also occurs as a high risk factor in this age group (10,11).
The negative effects of smoking on health are generally well studied, but, possibly due to challenges and inaccuracies in collecting data on smokers, only a limited number of studies have investigated the association between smoking and fractures on a national level. We hypothesized that smoking increases the risk of fractures directly, making bones prone to fractures, and indirectly, through increasing risk-taking behavior among smokers (12,13). As studies assessing fracture risk caused by smoking on the population level are lacking, studies with a large nationwide study sample should be performed. Thus, we investigated the fracture rate in smoking women of fertile-age and compared it with that of non-smoking women using data from nationwide registers.
Patients and methods
In this nationwide retrospective register-based cohort study, data from the National Medical Birth Register (MBR) was combined with data from the Care Register for Health Care. Both registers are maintained by the Finnish Institute for Health and Welfare. Data from both registers was then combined using the pseudonymized identification number of the mother. The study period was from January 1, 1998, to December 31, 2018.
Registers
The MBR contains information on pregnancies, delivery statistics, and perinatal outcomes of all births with a birthweight of ≥ 500 g or a gestational age ≥ 22 weeks, including maternal smoking habits. According to a study by Gissler et al. (14) the reliability of smoking status has been found to be good. The MBR has a high coverage and quality (the current coverage is nearly 100%) (15,16). We included every pregnancy between 1998 and 2013 leading to birth in women aged 15–44. In the MBR, smoking is categorized as either non-smoker, smoker during the 1st trimester of pregnancy but quitted, smoker throughout the pregnancy, or unknown. Women smoking during the 1st trimester of pregnancy, or in later trimesters, were included in the smoker group in our report. Women in the smoker group were compared with the non-smoker group.
The Care Register for Health Care contains information on all special healthcare visits during our study period. The coverage and quality of the Care Register for Health Care is good (17). Each fracture between 1998 and 2018 was included in this study. ICD-10 (International Classification of Diseases 10th revision) codes were used to identify fracture patients. Fractures of the lower arm, upper arm, spine, pelvis, hip or thigh, and lower leg were included.
Formation of study groups
Both groups, smokers and non-smokers, were linked with data found in the Care Register for Health Care. Pregnancies with unknown smoking status were excluded. Based on our hypothesis, the potential risk of fractures among smokers might be diverse, as it may be caused by weakened health of bone (osteoporosis, weakened circulation etc.) leading to a higher number of low-energy fractures (18), or by risky behavior, which has been found to be more common among people of lower socioeconomic status (SES) (12,13), leading to accident-proneness. Due to this hypothesis, we categorized women in 4 SES classes, low, middle, high, and undefinable, using the SES found in the MBR. The categorization of the SES is indicated in Table 1 (see Supplementary data). Pregnancies with missing SES (17%) were excluded from the analysis. 110,675 pregnancies with a smoking mother were found in the MBR. In 628,085 pregnancies the mother did not smoke (Figure 1).
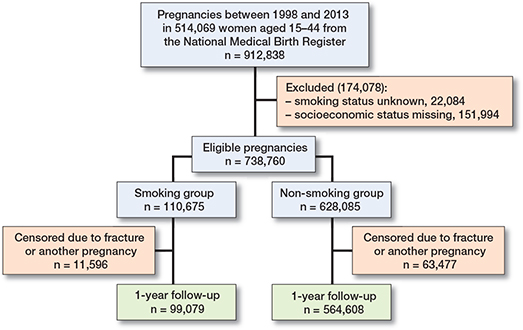
Figure 1. Flowchart of the study population. Data from the National Medical Birth Register was combined with data on the diagnosed fracture hospitalizations in the Care Register for Health Care.
Outcomes
The period of fracture hospitalization found in in the Care Register for Health Care was used to compare the risk of a woman suffering a fracture after giving birth. The total risk and the risk of fractures of different anatomic regions were the main outcomes. In addition, we analyzed the risk of polytraumas, for hospitalization period longer than 1 day (presumably more severe trauma), and risk of non-admitted fractures requiring a less than 1 day hospitalization period (including day surgery) with fracture diagnoses in only 1 anatomic region of the body (presumably non-severe trauma). Polytrauma was defined as 2 or more fracture ICD-10 diagnoses codes from at least 2 anatomic regions of the body during the same hospitalization period. This study is reported according to the STROBE guidelines (19).
Statistics
Continuous variables were reported as mean with standard deviation (SD) or as median with interquartile range (IQR) based on distribution of the data. Categorized variables were presented as absolute numbers and percentages. Kaplan–Meier survival curves were used to evaluate the absolute risk during the follow-up period. The Cox regression model was used to evaluate the risk of a fracture after pregnancy. Smokers were compared with non-smokers. The follow-up times were 1 and 5 years, starting from the day of giving birth found in the MBR. These follow-up times were chosen as the interests were in the risk of fractures during the lactation period and stay-at-home phase (approximately 1 year after giving birth) and the post-lactation period. The endpoint of the follow-up was 1 of the following events: the 1st fracture after giving birth, start of the next pregnancy, or the common endpoint of the follow-up, which was 1 or 5 years after giving birth, depending on the chosen follow-up time. The univariable and adjusted hazard for fractures was calculated. The multivariable model was adjusted for the age of the mother during pregnancy, as it is known to affect to the risk of fractures and SES category of the mother, to minimize the effect of background and behavioral differences. The results were interpreted with unadjusted hazard ratios (HRs), adjusted hazard ratios (aHRs), and 95% confidence intervals (CI). Proportional hazards assumption was tested using Schoenfeld residuals and the assumption was not violated in any tested model. Competing risks were handled using Efron’s method. Statistical significance was analyzed based on the 95% confidence intervals. Statistical analysis was performed using R version 4.0.3 (R Foundation for Statistical Computing, Vienna, Austria).
Sensitivity analyses
Sensitivity analysis with excluded patients due to missing SES was conducted for the Cox regression analysis (Table 5, see Supplementary data). In this analysis, women with missing SES were placed in their own SES category (“missing SES”) and the model was as in the main analyses.
In addition, sensitivity analysis using the multiple imputation techniques was performed. Best–best case, best–worst case, worst–best case, worst–worst case imputation, and data as observed were used to calculate grand means using the modified Rubin’s Rule (Table 6, see Supplementary data).
Ethics, funding, data sharing, and disclosures
Both registers, the National Medical Birth Register (MBR) and Care Register for Health Care, had the same unique pseudonymized identification number for each patient. The pseudonymization was done by the Finnish data authority Findata. The authors did not have access to the pseudonymization key as it is maintained by Findata. In accordance with Finnish regulations, no informed written consent was required because of the retrospective register-based study design and as the patients were not contacted. Permission for this data was granted by the Findata after evaluation of the study protocol (Permission number: THL/1756/14.02.00/2020). This study has not received funding. The authors declare no conflicts of interest. The data that supports the findings of this study is available from Findata, but restrictions apply to the availability of this data, which was used under license for the current study, and so is not publicly available. Data is, however, available from the authors upon reasonable request and with the permission of Findata (url: Findata.fi, email: info@Findata.fi). The corresponding author (MV) can be contacted for the data with a reasonable request.
Results
The prevalence of smokers among pregnant women stayed relatively stable during 1998–2012, ranging between 12% and 14%. However, after reaching its peak in 2012, the rate decreased to 10% in 2018 (Figure 2, see Supplementary data). Women who smoked were younger than their non-smoking counterparts at the time of delivery, with a mean age of 28 years (SD 6) among smokers and 30 years (SD 5) among non-smokers. A notably lower rate of women who smoked had been married during or before the pregnancy (37% vs. 66%). In the smoking group, there was also a notably higher rate of women of low SES (33% vs. 17%) and lower rate of high SES (6% vs. 22%) (Table 2). A higher rate of smoking women suffered a fracture in the following 1 year (0.3% vs. 0.2%) and 5 years after pregnancy (1.5% vs. 0.8%) (Table 3).
| Factor | Smoker group n = 110,675 | Non-smoker group n = 628,085 |
| Fracture during 1-year follow-up | 363 (0.3) | 1,196 (0.2) |
| Fracture during 5-year follow-up | 1,660 (1.5) | 5,238 (0.8) |
| Fracture location (after 5-year follow-up) a | ||
| Lower arm | 584 (35) | 2,305 (44) |
| Upper arm | 197 (12) | 604 (12) |
| Spine | 115 (6.9) | 247 (4.7) |
| Pelvis | 49 (3.0) | 101 (1.9) |
| Hip or thigh | 53 (3.2) | 110 (2.1) |
| Lower leg including ankle | 693 (42) | 1,907 (36) |
| a More than 1 location possible. | ||
Fractures of the lower arm, lower leg, and upper arm were the most common types of traumas. In the smoker group, 35% of fractures occurred in the lower arm, 42% in the lower leg, and 12% in the upper arm. Among non-smokers, 44% of fractures occurred in the lower arm, 36% in the lower leg, and 12% in the upper arm (Table 3).
The cumulative incidence plot showed that smokers had a higher fracture rate from the beginning. The curve showed a smaller increase for non-smoking women (Figure 3). The total fracture rate was higher among smoking women than among non-smokers during the 1-year follow-up (aHR 1.7, CI 1.5–2.0) and 5-year follow-up (aHR 1.7, CI 1.6–1.8). After the 1-year follow-up, the fracture rate for all anatomical regions except for the hip was higher among smokers than among non-smokers. The fracture rate was highest for the pelvis (aHR 2.2, CI 1.1–4.2) and spine (aHR 2.1, CI 1.3–3.4). After 5 years, the fracture rate was higher for all anatomic regions. The fracture rate was highest for hip or thigh fractures (aHR 2.4, CI 1.7–3.4), followed by spine fractures (aHR 2.3, CI 1.8–2.9), and pelvic fractures (aHR 2.1, CI 1.5–3.0).
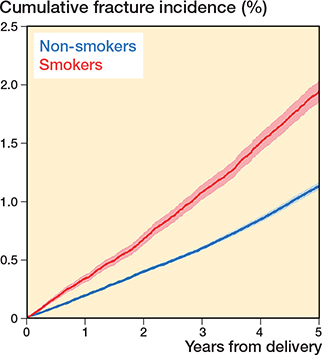
Figure 3. Cumulative incidence plot (with 95% CI) of fertile-aged women for the event of suffering a fracture after giving birth.
The risk of polytraumas among smoking women was higher after 5-year follow-up (aHR 2.3, CI 1.4–3.7). The risk of fractures requiring hospitalization for longer than 1 day was also higher after 1-year follow-up (aHR 2.1, CI 1.6–2.9) and after 5-year follow-up (aHR 2.0, CI 1.7–2.4) among smoking women. The risk of non-severe fractures (less than 1-day hospitalization period) was not as high as with severe fractures, but still higher among smoking women, the aHR being 1.8 (CI 1.6–2.0) after 1-year follow-up and 1.8 (CI 1.7–1.9) after 5-year follow-up (Table 4). All sensitivity analyses also showed a markedly increased risk of fractures among smokers (Tables 5 and 6, see Supplementary data).
| Fracture | 1-year follow-up | 5-year follow-up | ||
| HR (CI) | aHR (CI) a | HR (CI) | aHR (CI) a | |
| Total | 1.7 (1.5–2.0) | 1.7 (1.5–2.0) | 1.7 (1.6–1.8) | 1.7 (1.6–1.8) |
| Location of fracture | ||||
| Lower arm | 1.4 (1.1–1.7) | 1.4 (1.2–1.8) | 1.4 (1.3–1.5) | 1.4 (1.3–1.6) |
| Upper arm | 1.8 (1.3–2.6) | 1.8 (1.3–2.5) | 1.8 (1.5–2.1) | 1.7 (1.4–2.0) |
| Spine | 2.6 (1.7–4.0) | 2.1 (1.3–3.4) | 2.6 (2.0–3.2) | 2.3 (1.8–2.9) |
| Pelvis | 2.5 (1.3–4.7) | 2.2 (1.1–4.2) | 2.7 (1.9–3.8) | 2.1 (1.5–3.0) |
| Hip or thigh | 1.8 (0.9–3.4) | 1.8 (0.9–3.4) | 2.7 (1.9–3.7) | 2.4 (1.7–3.4) |
| Lower leg including | ||||
| ankle | 1.9 (1.6–2.3) | 1.9 (1.6–2.3) | 2.0 (1.8–2.2) | 2.0 (1.9–2.2) |
| Type of fracture | ||||
| Polytrauma | 0.8 (0.2–3.3) | 0.5 (0.1–2.3) | 3.0 (1.9–4.9) | 2.3 (1.4–3.7) |
| Severe b | 2.1 (1.6–2.9) | 2.1 (1.6–2.9) | 2.0 (1.7–2.3) | 2.0 (1.7–2.4) |
| Less severe c | 1.8 (1.6–2.0) | 1.8 (1.6–2.0) | 1.7 (1.6–1.8) | 1.8 (1.7–1.9) |
| a Adjusted for the age of the mother at the time of pregnancy and SES category. | ||||
| b Fractures with hospitalization period lasting > 1 day. | ||||
| c Fractures with < 1 day hospitalization (including day surgeries) and non-polytraumas. | ||||
Discussion
The main finding of this study was that smoking was associated with a higher fracture rate during the 1-year and 5-year follow-up time after giving birth when compared with non-smokers. After 5-year follow-up the risk was higher for all studied fractures in different anatomical regions, especially for the spine, pelvis, and hip or thigh. Also, the risk was higher for fractures considered as more severe (polytraumas and fractures requiring a longer hospitalization period) than for non-severe fractures (non-polytraumas and 1-day hospitalization period).
According to previous literature, a low SES has been overrepresented in trauma populations, but the exact reason behind this is unknown (13). In addition, according to the Finnish Institute for Health and Welfare (3), people who have a lower level of education smoke more than those with a higher level of education. Based on our data, there was a notably higher number of women with low SES in the group of smokers, which supports these finding in the previous literature. However, adjusting the model with categorized SES still showed a notably higher fracture rate among smokers, possibly indicating that the riskier behavior is not the only explanation behind the increased incidence of fractures among smoking women. In the elderly population, due to age-related skeletal fragility (20), polytraumas require less energy to occur (21), but in the fertile-aged population, polytraumas are known to be caused mostly by high-energy trauma mechanisms, such as traffic accidents and falls from a height (22). Adjusting the model for polytraumas with the age of the mother and SES, the aHR showed a greater decrease compared with crude HR for this model than for others. This could possibly mean that the increased number of injuries caused by behavioral background is a more important explanation for high-energy accidents causing injuries in multiple anatomic regions but less important for low-energy fractures among smoking women. In addition, it appears that during the lactation period mothers are at a smaller risk of severe injuries, as the number of polytraumas was truly low during 1-year follow-up.
The risk of non-severe fractures was also higher for smoking women but, based on our data, the reason behind this remains unclear, as these fractures could also be caused by injuries related to behavioral background. However, aHRs showed a notably higher risk of fractures among smoking women when the SES was considered. Smoking is known to be a strong risk factor for osteoporosis, due to the numerous ways it negatively affects bone health and metabolism (7,18). In addition, estrogen is the key regulator of bone metabolism (23), making women (especially oft premenopausal and postmenopausal age) at risk of osteoporosis (9,11). These 2 risk factors could make smoking women especially vulnerable to osteoporotic fractures. However, age is known to be a dominating risk factor for osteoporosis (24), making osteoporosis relatively rare among the fertile-aged population (25).
In general, the association between smoking and osteoporotic fractures based on our data is only speculative and the increased risk of fractures among smokers is most likely caused by the combined effect of numerous factors, such as more common risky behavior, weaker health of the musculoskeletal system caused by an unhealthier lifestyle, and possibly the direct weakening effects of smoking on the musculoskeletal system. However, as the results of this study are proving the association in a nationwide setting and the results showed a great increase in the risk of fractures, these results should be acknowledged by the clinician and used when encouraging the patient to quit smoking. In addition, the results of this study should encourage research on the etiology behind the increased risk using more precise datasets (whether the increased risk is caused by direct effects of smoking on bone health, or riskier behavior).
Due to challenges and inaccuracies in gathering data on smokers, the studies researching the association between smoking and fractures are made using a relatively small population or questionnaires (8,26,27). The strength of our study is the large nationwide register with a smoking status variable registered for each pregnancy during the study period, making it the most comprehensive data found regarding smoking by women in Finland. The register data used in our study is routinely collected using structured forms with national instructions, which ensures good coverage and reduces possible reporting and selection bias. (28). Furthermore, the coverage of both registers included in this study is high (15,17).
The main limitation of our study is residual confounding as there is no reason to believe that smoking in itself causes more polytrauma. Residual confounding may be the bone mineral density, other comorbidities, substance (alcohol, drugs etc.) abuse, and missing clinical information on the registered fractures (e.g., radiological finding, trauma mechanisms). As this information is not reported to the registers, a level of uncertainty on the severity of the traumas remains, as it is derived from the existence of fractures in multiple anatomical sites and the length of hospital stay. Also, a relatively high proportion of pregnancies (19%) were excluded from the analysis due to missing SES or smoking status. However, the excluded population is missing at random, and, based on our sensitivity analyses, this does not have a major impact on the results. Furthermore, the date of death and migration is not available based on our data, making it impossible to identify women lost to follow-up. Also, in terms of the risk of fractures, smoking status found in the MBR is not comprehensive as it does not expose those who did not admit their smoking during maternity clinic visits or contain any information on how much the person smokes. However, the reliability of smoking status in the MBR was over 92%, which makes it a reliable source (14).
Conclusion
Smoking among fertile women was associated with higher risk of fractures in all anatomic regions after 5 years of follow-up. Smoking was also associated with a higher risk of polytraumas, other more severe fractures, and less severe fractures.
- Jha P, MacLennan M, Chaloupka F J, et al. Global hazards of tobacco and the benefits of smoking cessation and tobacco taxes. In: Gelband H, Jha P, Sankaranarayanan R, Horton S, editors. Cancer: disease control priorities, 3d ed. (Volume 3). International Bank for Reconstruction and Development / World Bank; 2015. http://www.ncbi.nlm.nih.gov/books/NBK343639/. Accessed January 15, 2022.
- Jafari A, Rajabi A, Gholian-Aval M, Peyman N, Mahdizadeh M, Tehrani H. National, regional, and global prevalence of cigarette smoking among women/females in the general population: a systematic review and meta-analysis. Environ Health Prev Med. 2021; 26(1): 5. doi: 10.1186/s12199-020-00924-y.
- THL. Tobacco—THL. Finnish Institute for Health and Welfare (THL), Finland. Published 2018. https://thl.fi/en/web/alcohol-tobacco-and-addictions/tobacco. Accessed January 15, 2022.
- Tobacco. https://www.who.int/news-room/fact-sheets/detail/tobacco. Accessed September 16, 2022.
- Bartal M. Health effects of tobacco use and exposure. Monaldi Arch Chest Dis Arch Monaldi Mal Torace 2001; 56(6): 545-54.
- Sherman C B. Health effects of cigarette smoking. Clin Chest Med 1991; 12(4): 643-58.
- Al-Bashaireh A M, Haddad L G, Weaver M, Chengguo X, Kelly D L, Yoon S. The effect of tobacco smoking on bone mass: an overview of pathophysiologic mechanisms. J Osteoporos 2018; 2018: 1206235. doi: 10.1155/2018/1206235.
- Hernigou J, Schuind F. Tobacco and bone fractures: a review of the facts and issues that every orthopaedic surgeon should know. Bone Joint Res 2019; 8(6): 255-65. doi: 10.1302/2046-3758.86.BJR-2018-0344.R1.
- Keen M U, Reddivari A K R. Osteoporosis in females. In: StatPearls. StatPearls Publishing; 2022. http://www.ncbi.nlm.nih.gov/books/NBK559156/. Accessed January 17, 2022.
- Bischoff L, Derk C T. Premenopausal osteoporosis. Minerva Med 2008; 99(1): 55-63.
- Vondracek S F, Hansen L B, McDermott M T. Osteoporosis risk in premenopausal women. Pharmacotherapy 2009; 29(3): 305-17. doi: 10.1592/phco.29.3.305.
- Hiscock R, Bauld L, Amos A, Fidler J A, Munafò M. Socioeconomic status and smoking: a review. Ann N Y Acad Sci 2012; 1248: 107-23. doi: 10.1111/j.1749-6632.2011.06202.x.
- Geckova A, van Dijk J P, Groothoff J W, Post D. Socio-economic differences in health risk behaviour and attitudes towards health risk behaviour among Slovak adolescents. Soz Praventivmed 2002; 47(4): 233-9. doi: 10.1007/BF01326404.
- Gissler M, Teperi J, Forssas E, Hemminki E. Syntymärekisterin Luotettavuustutkimus 1991; 1993.
- Gissler M, Shelley J. Quality of data on subsequent events in a routine medical birth register. Med Inform Internet Med 2002; 27(1): 33-8. doi: 0UB69R4X61VDGCDA [pii].
- Gissler M, Teperi J, Hemminki E, Meriläinen J. Data quality after restructuring a national medical registry. Scand J Soc Med 1995; 23(1): 75-80. doi: 10.1177/140349489502300113.
- Sund R. Quality of the Finnish Hospital Discharge Register: a systematic review. Scand J Public Health 2012; 40(6): 505-15. doi: 10.1177/1403494812456637.
- Chen J S, Hogan C, Lyubomirsky G, Sambrook P N. Women with cardiovascular disease have increased risk of osteoporotic fracture. Calcif Tissue Int 2011; 88(1): 9-15. doi: 10.1007/s00223-010-9431-7.
- Elm E von, Altman D G, Egger M, Pocock S J, Gøtzsche P C, Vandenbroucke J P, STROBE Initiative. The strengthening the reporting of observational studies in epidemiology (STROBE) statement: guidelines for reporting observational studies. J Clin Epidemiol 2008; 61(4): 344-9. doi: 10.1016/j.jclinepi.2007.11.008.
- Burr D B. Changes in bone matrix properties with aging. Bone 2019; 120: 85-93. doi: 10.1016/j.bone.2018.10.010.
- de Vries R, Reininga I H F, Pieske O, Lefering R, El Moumni M, Wendt K. Injury mechanisms, patterns and outcomes of older polytrauma patients: an analysis of the Dutch Trauma Registry. PloS One 2018; 13(1): e0190587. doi: 10.1371/journal.pone.0190587.
- van Breugel J M M, Niemeyer M J S, Houwert R M, Groenwold R H H, Leenen L P H, van Wessem K J P. Global changes in mortality rates in polytrauma patients admitted to the ICU: a systematic review. World J Emerg Surg 2020; 15(1): 55. doi: 10.1186/s13017-020-00330-3.
- Cauley J A. Estrogen and bone health in men and women. Steroids 2015; 99(Pt A): 11-15. doi: 10.1016/j.steroids.2014.12.010.
- Jakobsen A, Laurberg P, Vestergaard P, Andersen S. Clinical risk factors for osteoporosis are common among elderly people in Nuuk, Greenland. Int J Circumpolar Health 2013; 72: 19596. doi: 10.3402/ijch.v72i0.19596.
- Clynes M A, Harvey N C, Curtis E M, Fuggle N R, Dennison E M, Cooper C. The epidemiology of osteoporosis. Br Med Bull 2020; 133(1): 105-17. doi: 10.1093/bmb/ldaa005.
- Kanis J A, Johnell O, Oden A, Johansson H, De Laet C, Eisman J A, et al. Smoking and fracture risk: a meta-analysis. Osteoporos Int 2005;16(2): 155-62. doi: 10.1007/s00198-004-1640-3.
- Vestergaard P, Mosekilde L. Fracture risk associated with smoking: a meta-analysis. J Intern Med 2003; 254(6): 572-83. doi: 10.1111/j.1365-2796.2003.01232.x.
- THL. Perinatal statistics: parturients, delivers and newborns—THL; 2018. https://thl.fi/en/web/thlfi-en/statistics-and-data/data-and-services/register-descriptions/newborns.
Supplementary data
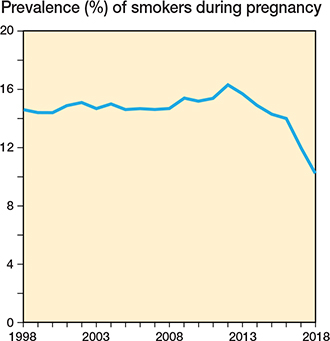
Figure 2. Prevalence of smokers during pregnancy of all pregnancies in Finland during 1998–2018. Women smoking during 1st trimester of pregnancy, or in later trimesters, were considered smokers in this study.
| Fracture | 1-year follow-up | 5-year follow-up | ||
| HR (CI) | aHR (CI) a | HR (CI) | aHR (CI) a | |
| Total | 1.7 (1.5–2.0) | 1.7 (1.5–1.9) | 1.7 (1.6–1.8) | 1.7 (1.7–1.8) |
| Location of fracture | ||||
| Lower arm | 1.4 (1.1–1.7) | 1.5 (1.2–1.8) | 1.4 (1.3–1.5) | 1.5 (1.3–1.6) |
| Upper arm | 1.9 (1.3–2.6) | 1.8 (1.3–2.4) | 1.8 (1.5–2.1) | 1.7 (1.5–2.0) |
| Spine | 2.6 (1.7–4.0) | 2.1 (1.4–3.1) | 2.6 (2.0–3.2) | 2.3 (1.9–2.8) |
| Pelvis | 2.5 (1.3–4.7) | 1.7 (0.9–3.2) | 2.7 (1.9–3.8) | 2.0 (1.5–2.8) |
| Hip or thigh | 1.8 (0.9–3.4) | 2.1 (1.2–3.9) | 2.7 (1.9–3.7) | 2.2 (1.6–3.0) |
| Lower leg including | ||||
| ankle | 1.9 (1.6–2.3) | 1.8 (1.5–2.2) | 2.0 (1.8–2.2) | 2.0 (1.8–2.2) |
| Type of fracture | ||||
| Polytrauma | 0.8 (0.2–3.3) | 0.4 (0.1–1.9) | 3.1 (1.9–4.9) | 2.2 (1.4–3.4) |
| Severe b | 2.1 (1.6–2.9) | 2.2 (1.7–2.9) | 2.0 (1.7–2.3) | 2.0 (1.8–2.3) |
| Less severe c | 1.8 (1.6–2.0) | 1.8 (1.6–2.0) | 1.7 (1.6–1.8) | 1.8 (1.6–2.0) |
| a Adjusted for the age of the mother at the time of pregnancy and SES category. | ||||
| b Fractures with hospitalization period lasting > 1 day. | ||||
| c Fractures with < 1 day hospitalization (including day surgeries) and non-polytraumas. | ||||
| Fracture | 1-year follow-up | 5-year follow-up | ||
| HR (CI) | aHR (CI) a | HR (CI) | aHR (CI) a | |
| Total | 1.7 (1.5–2.0) | 1.7 (1.5–3.0) | 1.7 (1.6–1.8) | 1.7 (1.6–1.8) |
| Location of fracture | ||||
| Lower arm | 1.4 (1.1–1.7) | 1.4 (1.2–1.8) | 1.4 (1.3–1.5) | 1.4 (1.3–1.6) |
| Upper arm | 1.9 (1.3–2.6) | 1.8 (1.3–2.5) | 1.8 (1.5–2.1) | 1.7 (1.4–2.0) |
| Spine | 2.6 (1.7–4.0) | 2.1 (1.3–3.4) | 2.6 (2.0–3.2) | 2.3 (1.8–2.9) |
| Pelvis | 2.5 (1.3–4.7) | 2.2 (1.1–4.3) | 2.7 (1.9–3.8) | 2.1 (1.5–3.0) |
| Hip or thigh | 1.8 (0.9–3.4) | 1.8 (0.9–3.5) | 2.7 (1.9–3.7) | 2.1 (1.5–3.0) |
| Lower leg including | ||||
| ankle | 1.9 (1.6–2.3) | 1.9 (1.6–2.3) | 2.0 (1.8–2.2) | 2.0 (1.9–2.2) |
| Type of fracture: | ||||
| Polytrauma | 0.8 (0.2–3.3) | 0.5 (0.1–2.8) | 3.1 (1.9–4.9) | 2.2 (1.4–3.6) |
| Severe b | 2.1 (1.6–2.9) | 2.1 (1.6–2.9) | 2.0 (1.7–2.3) | 2.0 (1.7–2.4) |
| Less severe c | 1.8 (1.6–2.0) | 1.8 (1.6–2.0) | 1.7 (1.6–1.8) | 1.7 (1.7–1.9) |
| a–c see Table 5 | ||||