Proximal femoral fractures in children: incidence, complications, and functional outcomes—a population-based study from Finland
Sini-Tuuli KOIVISTO 2,4, Ilkka HELENIUS 1,3,4, Antti STENROOS 1,4, Juho-Antti AHOLA 1,4, and Topi LAAKSONEN 1,4
1 Department of Pediatric Orthopaedics and Traumatology, University of Helsinki and Helsinki New Children’s Hospital, Helsinki; 2 Faculty of Medicine, University of Helsinki, Helsinki; 3 Department of Orthopaedics and Traumatology, University of Helsinki and Helsinki University Hospital, Helsinki; 4 Finnish Pediatric Orthopaedics Research Group (FiPO), Helsinki, Finland
Background and purpose — Pediatric proximal femoral fractures are rare and frequently complicated fractures with avascular necrosis (AVN), nonunion, deformity, leg-length discrepancy (LLD), and premature physeal closure (PPC). Our aim was to describe the incidence, complications and functional outcomes.
Methods — In this register-based study from a 10-year period (2014–2023) we identified 51 non-pathological proximal femoral fractures from the KIDS Fracture Tool database. Statistical yearbooks of Helsinki were utilized to estimate annual incidence. We used interviews and Oxford Hip Scores (OHS) for functional outcome assessment. If any symptom or functional deficit was described, or if Oxford Hip Score (OHS) was < 41, patients were also invited for clinical examination and radiography.
Results — 51 patients with a proximal femoral fracture (31 boys) were identified representing 0.2% (51/21,121) of all child fractures with a population-based annual incidence of 1.7/100,000 children. We interviewed 46/51 of the patients or their guardians via telephone. 6/46 were invited for clinical examination and radiography. Median follow-up of contacted patients was 4 (range 1–9.5) years. Complications occurred in 9/20 patients with collum and trochanteric fractures (pain from osteosynthesis 4, AVN 3, nonunion 1, coxa vara 1, LLD 1, PPC 0) and in 7/31 with subtrochanteric fractures (pain from osteosynthesis 5, misplaced pins 2, angular deformity 1, peri-implant fracture 1). All underwent reoperation. The median OHS was 48 (interquartile range 47–48) at last follow-up. Functional outcomes were impaired in 3 patients. All 3 had AVN.
Conclusion — The incidence of non-pathological pediatric proximal femoral fractures is low. Despite frequent complications, impaired functional outcomes concerned only patients with AVN at median 4-year follow-up.
Citation: Acta Orthopaedica 2025; 96: 726–734. DOI: https://doi.org/10.2340/17453674.2025.44752.
Copyright: © 2025 The Author(s). Published by MJS Publishing – Medical Journals Sweden, on behalf of the Nordic Orthopedic Federation. This is an Open Access article distributed under the terms of the Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0/)
Submitted: 2025-03-03. Accepted: 2025-08-26. Published: 2025-09-30.
Correspondence: sini-tuuli.koivisto@helsinki.fi
STK: study design, data acquisition, statistics, manuscript preparation, correspondence. IH: study design, manuscript preparation. AS: study design, data acquisition, manuscript preparation. JAA: data acquisition, manuscript preparation. TL: study design, data acquisition, manuscript preparation,
Handling co-editors: Cecilia Rogmark and Robin Christensen
Acta thanks Ole Rahbek and other anonymous reviewers for help with peer review of this manuscript.
Proximal femoral fractures in pediatric populations are rare, and comprise < 1% of all fractures [1]. A population-based incidence of 0.5–4/100,000 children has been reported in a binational study including pathological and non-pathological fractures [2]. In contrast to femoral shaft fractures, proximal fractures occur more often in older children [3]. Increasing age predicts both higher incidence and higher involvement of boys [2]. These injuries often follow high-energy traumas (motor vehicle collisions, falls, sports), while low-energy fractures are associated with predisposing conditions or lesions, such as bone cysts [1].
Management of collum, trochanteric, and subtrochanteric fractures emphasizes reduction and fixation [4,5]; nevertheless, these fractures are associated with a high risk of complications [6]. This introduces the risk of long-term morbidity, and understanding these injuries’ significance to the patient in the longer term is important. Few studies have focused on reporting outcomes: Ratliff’s criteria [7] have been used for reporting outcomes for collum and trochanteric fractures, and outcomes for subtrochanteric fractures with Flynn’s criteria have been reported even less [8,9]. Most previous outcome reports are based on retrospective data and rely more on radiographic findings [6,8-11]. The aim of our study is to describe the incidence and complications, and to assess functional outcomes, by contacting those treated for pediatric proximal femoral fracture in a population-based study.
Methods
Study design
This is a descriptive, register-based follow-up study investigating population-based characteristics and outcomes of pediatric proximal femoral fractures. Eligible proximal femoral fractures from a 10-year-study period (January 1, 2014–December 31, 2023) were identified using the KIDS Fracture Tool. Reporting adhered to the STROBE guidelines [12].
Setting
This study included pediatric proximal femoral fracture patients treated at the New Children’s Hospital during 2014–2023, where the management of these fractures is centralized. Our patients are from the Province of Uusimaa, which includes Helsinki capital region (Helsinki, Espoo, Vantaa, Kauniainen) and smaller municipalities. It is the only tertiary-level hospital in Helsinki capital region and the sole provider of on-call pediatric orthopedic treatment in Finland. The hospital services are accessible to all in our public-funded healthcare system.
Data collection
The study population was identified using the KIDS Fracture Tool, which is an electronic database designed for pediatric fracture management and quality monitoring. This tool has prospectively recorded data (age, home municipality, injury mechanism, diagnosis, management, complications, follow-up visits) on fractures diagnosed in patients aged 15 years or younger since 2014 [13]. The total number of all children’s fractures during the study period was obtained from the KIDS Fracture Tool. Yearly counts of the pediatric population (< 16 years) between 2014 and 2023 in Helsinki capital region (Helsinki, Espoo, Vantaa, Kauniainen) were obtained from the Statistical Yearbook of Helsinki for annual incidence estimation [14]. Details from radiographs (e.g., fracture location, dislocation, angulation) and clinical contacts (e.g., status, recovery process) were recorded from patient records. Complications (e.g., AVN, nonunion, PPC, LLD, angular deformities) were re-evaluated from follow-up radiographs and/or computed tomography scans, if available. Outcome data was collected from patient interviews via telephone and, if needed, clinical examination and radiography.
Study population
We reviewed radiographs of all proximal femoral fractures and diaphyseal fractures registered in the KIDS Fracture Tool to confirm diagnosis and eligibility. Patients with pathological fractures, slipped capital femoral epiphysis, stress fractures, or avulsion fractures were excluded. Collum and trochanteric fractures were classified using the Delbet classification, which includes transepiphyseal, transcervical, basicervical, and intertrochanteric fractures denoted by Delbet types I–IV, respectively [15]. Subtrochanteric fractures were defined as those occurring entirely within 20% of the total femoral length below the lesser trochanter (Figure 1). Subtrochanteric fractures were classified into complete and incomplete (torus, greenstick) fractures. Patients were followed for a minimum of 1 year and no patient was excluded due to this criterion.

Figure 1. The area located within 20% of the total length of the femur below the lesser trochanter, defines the subtrochanteric fracture area. Subtrochanteric fractures by our definition should be entirely confined to this area, not only extend to it.
Variables
Injury mechanism was categorized into various falls (ground level and from a height), motor vehicle accidents (MVA), sports accidents, and others. Injury mechanisms were categorized into 3 levels of energy: (i) low energy (ground-level falls), (ii) moderate energy (MVAs at speeds below 30 km/hour or falls from heights under 3 meters), and (iii) high energy (MVAs exceeding 30 km/hour or falls from substantial heights). Dislocation was classified as non-displaced (≤ 2 mm) or displaced (> 2 mm) in either plane. AVN was defined as post-traumatic presentation of sclerosis, subchondral lucency, and femoral head collapse, and then further graded to Ratliff’s AVN categories I–III [7]. Nonunion was defined as presence of an unhealed fracture at 6 months [16]. PPC was defined as the presence of a physeal bar or bony bridge on CT in the absence of physiological physeal closure. Coxa vara and varus/valgus malunion in the subtrochanteric region were defined as 10° difference compared with the healthy side. LLD was defined as ≥ 2 cm difference between limbs [17].
Outcomes
We attempted to contact all patients, or their guardians, if patients were < 18 years, to assess outcomes via telephone. Hip function was evaluated using the Oxford Hip Score (OHS) questionnaire (certified Finnish translation) [18]. The OHS assesses arthritis pain and functional deficit, ranging from 0 (worst outcome) to 48 (best outcome). Additionally, patients were invited to provide subjective descriptions of any pain, functional deficit, or dissatisfaction with the cosmetic outcome of their treatment. Those with OHS ≤ 41 or those reporting significant pain-related, functional, or cosmetic issues were invited for clinical follow-up and radiography. OHS > 41 was considered as a good result, as this represents the most conservative value found in the literature to denote the best outcome category [19].
Statistics
Counts, percentages, and median with range or interquartile range (IQR) were used as descriptive statistics. Pairwise deletion was used for missing values. The 10-year cumulative annual incidence rates for all proximal femoral fractures, collum and trochanteric fractures, and subtrochanteric fractures were calculated for Helsinki capital area (Helsinki, Espoo, Vantaa, Kauniainen). Statistics were compiled using Microsoft Excel (Microsoft Corp, Redmond, WA, USA).
Ethics, use of AI, funding, and disclosures
The study protocol was approved by the Helsinki University Hospital Review Board (HUS/564/2024). The KIDS Fracture Tool is linked to our electronic medical records, and written consent was not needed from parents for this register-based inquiry. Verbal informed consent was requested during interview. AI was not utilized. Author STK received a grant from the Finnish Medical Foundation to enable full-time working and declares no conflicts of interest. The other authors have not received any funding and declare no conflicts of interest. Complete disclosure of interest forms according to ICMJE are available on the article page, doi: 10.2340/17453674.2025.44752
Results
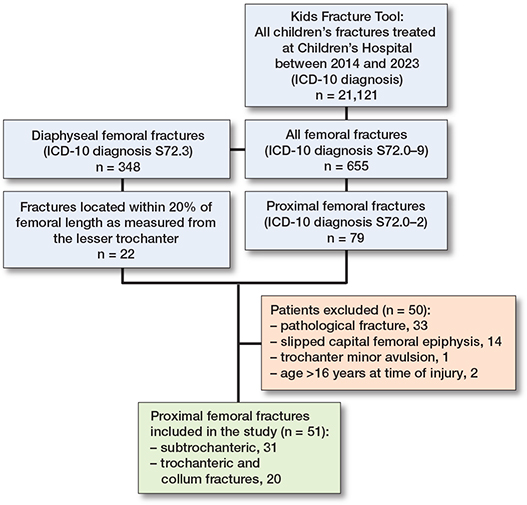
During the 10-year-study period we found 79 proximal femoral factures and 348 diaphyseal femoral fractures from the KIDS Fracture Tool in the Province of Uusimaa, including Helsinki (Figure 2). Of these, 51 proximal femoral fractures (31 boys) met the inclusion criteria for the study (Figure 2). They comprised 18 collum, 2 trochanteric, and 31 subtrochanteric femoral fractures. The median age was 10.1 years (IQR 3.7–14.3). Proximal femoral fractures represented 0.2% (51/21,121) of all children’s fractures in the Province of Uusimaa. The population-based annual incidence was 1.7/100,000 in Helsinki capital area. The median follow-up period of all 51 patients was 3.6 years (range 1–9.5), and the median follow-up period of the 46 contacted patients was 4 years (range 1.1–9.5).
Collum and trochanteric fractures
20 children (11 boys) presented with collum (n = 18) and trochanteric (n = 2) fractures. The fracture distribution according to Delbet classification from I–IV was 1, 11, 6, and 2, respectively. The median age was 13.5 years (IQR 10.5–15.3). The population-based annual incidence was 0.6/100,000 children. The most frequent injury mechanisms were 9 traffic accidents and 5 falls from a height (Table 1). 14 patients’ fractures were displaced: 1 with Delbet I, 7 with Delbet II, 5 with Delbet III, and 1 with Delbet IV fractures. In 2 patients, a non-dislocated and a 3 mm dislocated fracture were first unnoticed from plain radiographs, delaying diagnosis. 2 non-dislocated fractures were managed with cast immobilization in 1.3- and 8.7-year-old patients. 18 were managed with open reduction and internal fixation (ORIF) (Table 2).
| Mechanism of injury | ||||||||||||
| Factor | n | Median age (range) | Various falls | Traffic | Sport | Other | Injury energy | Associated injuries a | Treated < 24 hours | |||
| ground | height | Low | Moderate | High | ||||||||
| Collum and trochanteric fractures | ||||||||||||
| Delbet I | 1 | 13.5 | 1 | 1 | 1 | |||||||
| Delbet II | 11 | 12.4 (8.7–15.5) | 1 | 2 | 5 | 3 | 2 | 6 | 3 | 3 | 8 | |
| Delbet III | 6 | 14.9 (12.0–15.6) | 3 | 3 | 2 | 4 | 4 | 4 | ||||
| Delbet IV | 2 | 8.2 (1.3–15.1) | 1 | 1 | 1 | 1 | 1 | 2 | ||||
| Total | 20 | 13.5 (1.3–15.6) | 3 | 5 | 9 | 3 | 4 | 8 | 8 | 8 | 15 | |
| Subtrochanteric fractures | ||||||||||||
| Complete | 25 | 9.5 (1.9–15.1) | 4 | 10 | 5 | 6 | 6 | 16 | 3 | 1 | 22 | |
| Torus | 5 | 1.8 (1–2.8) | 2 | 3 | 5 | 4 | ||||||
| Greenstick | 1 | 1.6 | 1 | 1 | 1 | |||||||
| Total | 31 | 7.6 (1–15.1) | 5 | 12 | 5 | 6 | 3 | 12 | 16 | 3 | 1 | 27 |
| Total | 51 | 10.1 (1–15.6) | 8 | 17 | 14 | 9 | 3 | 16 | 24 | 11 | 9 | 42 |
| a 4 patients suffered multiple associated fractures and internal organ injuries, 4 suffered from 1 other fracture, and 1 sustained laceration wound only. | ||||||||||||
| Factor | n | Median age (range) | Median dislocation, mm (range) a | ||||
| Management of collum and trochanteric fractures | Delbet I | Delbet II | Delbet III | Delbet IV | |||
| Cast in situ | 2 | 5 (1.3–7.8) | 1 (0–2) | 1 | 1 | ||
| PHP | 2 | 10.6 (8.8–12.4) | 23.5 (16–31) | 1 | 1 | ||
| DHS | 7 | 14.7 (12.1–15.5) | 15 (0–35) | 4 | 3 | ||
| Cannulated screws | 8 | 13.9 (8.9–15.6) | 10 (0–26) | 1 | 5 | 2 | |
| LFN | 1 | 15.1 | 50 | 1 | |||
| Total | 20 | 13.5 (1.3–15.6) | 14.5 (0–50) | 1 | 11 | 6 | 2 |
| Management of subtrochanteric fractures | Complete subtrochanteric | Torus | Greenstick | ||||
| Limited weight-bearing | 2 | 1.9 (1–2.8) | 0 | 2 | |||
| Cast in situ | 2 | 1.3 (1–1.6) | 0 | 1 | 1 | ||
| MUA and cast in situ | 5 | 1.9 (1.8–3.7) | 4 (0–18) | 3 | 2 | ||
| Plate (LCP = 6, PHP = 5 c) | 11 | 9.3 (2.8–12.9) | 37 (7–49) | 11 | |||
| FIN | 7 | 9.5 (7.1–11) | 25 (8–45) | 7 | |||
| Locking nail (ALFN = 3, LFN = 1) | 4 | 14.9 (14.5–15.1) | 43 (12–100) | 4 | |||
| Total | 31 | 7.6 (1–15.1) | 9 (0–100) | 25 | 5 | 1 | |
| a 4 patients did not have lateral plane radiographs to evaluate sagittal displacement. b 6 patients did not have lateral plane radiographs to evaluate sagittal displacement, and 1 patient did not have AP-plane radiographs to evaluate coronal displacement. c One 2.8-year-old had preceding 7-day traction before PHP fixation. ALFN: adolescent lateral femoral nail; DHS: dynamic hip screw; FIN: flexible intramedullary nails; LCP: locking compression plate; LFN: lateral femoral nail; MUA: manipulation under anesthesia; PHP: pediatric hip plate. |
|||||||
Complications occurred in 9/20 patients during follow-up (Table 3). All complications occurred to patients with Delbet II fracture. 8/9 of these patients underwent at least 1 unplanned reoperation, and in 1/9 patient reoperation is yet to come. Complications included 4 removals of osteosynthesis material due to pain, 3 AVNs, 1 nonunion, 1 coxa vara (from AVN), 1 hardware failure, and 1 LLD (from AVN), and 0 PPCs (Table 3). All AVNs were noticed 12 to 14 weeks post-injury.
| Number | Sex, age | Fracture type | Mechanism of injury and associated injuries | Dislocation (mm) | Treatment, fixation, and timing | Complication | Reoperation | OHS | Total follow-up (years) |
| 1 | Girl, 12.4 | Delbet II | MVA, distal femur fracture | 15 | DHS < 24 hours | Ratliff I—AVN, loss of alignment, coxa vara, LLD | Re-fixation with cannulated screws and removal of screws | 47 | 5.4 |
| 2 | Girl, 10.1 | Delbet II | Horse-riding accident | 23 | Cannulated screws < 24 hours | Ratliff II—AVN | Underwent THA | 14 | 1.4 |
| 3 | Girl, 8.7 | Delbet II | Horse-riding accident, clavicle fracture | ≤ 2 b | Cast in situ, cannulated screws 12 days post-injury due to loss of reduction | Ratliff II—AVN | Not yet Further management strategy of AVN is still under consideration | 42 | 1.3 |
| 4 | Boy, 14.3 | Delbet II | Ski-jumping accident | 20 | Cannulated screws < 12 hours | Non-union | DHS fixation due to non-union | 48 | 9.1 |
| 5 | Boy, 8.9 | Delbet II | Soccer | 26 | Cannulated screws < 24 hours | Hardware failure | Replacement with DHS fixation | 48 | 1 |
| 6 | Girl, 8.8 | Delbet II | Ski-jumping accident | 31 | PHP < 24 hours | Pain | Unplanned OR | NA a | 1.9 |
| 7 | Boy, 15.5 | Delbet II | Moped accident | ≤ 2 b | DHS < 24 hours | Pain | Unplanned OR | 48 | 4.8 |
| 8 | Boy, 15.5 | Delbet II | Bike accident | 22 | Screw fixation < 24 hours | Pain | Unplanned OR | 42 | 2.6 |
| 9 | Boy, 13.4 | Delbet II | Bike accident, wrist fracture | ≤ 2 b | Initially missed diagnosis, DHS 30 days later | Missed diagnosis, pain | Unplanned OR | 48 | 7.2 |
| 10 | Boy, 10.5 | CS | Swing accident | 47 | LCP | Multiple peri-implant fractures | Multiple redo surgeries | NA a | 3.1 |
| 11 | Girl, 9.5 | CS | Quad bike accident | 28 | FIN | Suboptimal pin placement, varus deformity, and pain | Redo surgery x2, unplanned OR | 48 | 9.1 |
| 12 | Boy, 7.6 | CS | Sledding accident | 45 | FIN | Suboptimal pin placement | Redo surgery | 48 | 5 |
| 13 | Girl 7.2 | CS | Downhill skiing accident | 8 | FIN | Pain | Unplanned OR | 45 | 4.3 |
| 14 | Boy, 9.8 | CS | Sledding accident | 44 | FIN | Pain | Unplanned OR | 48 | 2.9 |
| 15 | Boy, 10.9 | CS | Downhill skiing | 25 | FIN | Pain | Unplanned OR | 48 | 7.8 |
| 16 | Boy, 9.7 | CS | MVA | 32 | LCP | Pain, whilst excessive scar tissue resection | Unplanned OR | 48 | 1.7 |
| a Not available due to inability to reach patient. b Non-dislocated AVN: avascular necrosis of the femoral head as classified by Ratliff into types I–III; CS: Complete subtrochanteric DHS: dynamic hip screw; FIN: flexible intramedullary nail; LCP: locking compression plate; LLD: leg-length discrepancy; MVA: motor vehicle accident; OR: osteosynthesis removal; PHP: pediatric hip plate; THA: total hip arthroplasty. |
|||||||||
Subtrochanteric fractures
31 children (20 boys) with a median age of 7.6 years (IQR 2.8–10.9) presented with subtrochanteric fractures. The population-based annual incidence was 1.1/100,000 children. The most frequent injury mechanisms were 12 falls from a height and 5 sports accidents traffic (see Table 1). All complete fractures (25/31) were displaced. 9 subtrochanteric fractures were treated by cast immobilization. 21 complete fractures underwent ORIF and 1 closed reduction and internal fixation (CRIF) (see Table 2).
Complications occurred in 7/31 patients (see Table 3). All complications occurred to patients with complete subtrochanteric fractures, and they underwent at least 1 unplanned reoperation. Complications included 5 removals of osteosynthesis due to pain, 1 varus malunion, 2 suboptimal pin placements, and 1 sustaining multiple peri-implant fractures.
Outcomes
We contacted 46/51 (90%) patients: 18 with collum and trochanteric and 28 with subtrochanteric fractures. Their median OHS was 48 (IQR 47–48), and outcome impairments were found in 3 patients, all with AVN: patients 1, 2, and 3 (Tables 3 and 4). 7 patients were invited for clinical examination and radiography due to subjective concern in the affected hip/limb (7/7) and due to OHS ≤ 41 (1/7). These subjective concerns were interpreted as relevant to preceding trauma or its management in 2 patients with AVN (nos 2 and 3) and in 1 patient with prominent osteosynthesis (no. 7). Patient no. 2 scored an OHS of only 14 (Table 4).
| Number | Sex, age | Fracture type | Injury mechanism | Treatment and complications | OHS | Follow-up (years) |
| 2 | Girl, 10.1 | Delbet II | Horse-riding accident | Cannulated screws fixation within 24 hours. Developed AVN | 14 | 1.4 |
| Patient’s concern: Stiffness, abnormal gait, inability to bear weight due to pain. | ||||||
| Clinical findings: Abnormal gait, ROM a: hip flexion 20°, internal and external rotations absent. Hip extension 0°. In extended hip, internal rotation 10°, external rotation 30°. | ||||||
| Radiography: AVN, femoral head partially collapsed. | ||||||
| Conclusion: Severely disabling AVN. Soon after our clinical examination the patient underwent THA. | ||||||
| 3 | Girl, 8.7 | Delbet II | Horse-riding accident | Cast in situ, cannulated screw 12 days post-injury due to loss of reduction. Developed AVN | 42 | 1.3 |
| Patient’s concern: Abnormal gait which is accentuated at distances > 200 m. No rest pain or need for painkillers. | ||||||
| Clinical findings: Abnormal gait. ROM: hip flexion 130°, internal rotation 40°, external rotation 30°, hip extension 0°. In extended hip, external rotation 0°. | ||||||
| Radiography: AVN, femoral head partially collapsed. | ||||||
| Conclusion: Absence of hip extension contributes to the abnormal gait. Will require further surgery. Management strategy of AVN still under consideration. | ||||||
| 7 | Boy, 15.5 | Delbet II | Moped accident | DHS, now wants plate removal | 48 | 4.8 |
| Patient’s concern: Post-exertional abnormal sensation distal to trochanter major. | ||||||
| Clinical findings: Normal hip function. Slim patient, DHS fixation is palpable. | ||||||
| Radiography: No findings. | ||||||
| Conclusion: Excellent hip recovery, osteosynthesis likely bothers, will proceed with removal. | ||||||
| 8 | Boy, 15.5 | Delbet II | Bike accident | Cannulated screws removed due to pain | 42 | 2.6 |
| Patient’s concern: Pain along gluteal region, especially after immobilization. | ||||||
| Clinical findings: Normal hip function | ||||||
| Radiography: No findings. | ||||||
| Conclusion: Excellent hip recovery. Able to participate in various sports. Symptoms seem unrelated to hip trauma. | ||||||
| 17 | Girl, 15.3 | Delbet III | MVA, multiple fractures | DHS | 45 | 3.5 |
| Patient’s concern: Occasional hip pain and stiffness. | ||||||
| Clinical findings: Normal hip function. | ||||||
| Radiography: Prominent lesser trochanter. | ||||||
| Conclusion: Excellent hip recovery. Currently at renovation-related work the hip does not bother or cause limitations Symptoms seem unrelated to hip trauma. | ||||||
| 11 | Girl, 9.5 | CS | Quad bike accident | FIN, suboptimal pin placement, osteosynthesis removal due to pain | 48 | 9.1 |
| Patient’s concern: Affected hip and leg seem weaker at sports activities. | ||||||
| Clinical findings: 10–15° internal rotation deficit in affected hip. | ||||||
| Radiography: 11° varus malunion. | ||||||
| Conclusion: Excellent hip recovery. Reported weakness seems unrelated to hip trauma. | ||||||
| 13 | Girl, 7.2 | CS | Downhill skiing | FIN, osteosynthesis removal due to pain | 45 | 4.3 |
| Patient’s concern: Pain in ipsilateral knee and heel. | ||||||
| Clinical findings: Normal hip function Affected leg 10 mm longer. Palpation tenderness in the heel. | ||||||
| Radiography: No findings. | ||||||
| Conclusion: Excellent hip recovery. Limb discrepancy clinically insignificant. Symptoms seem nunrelated to hip trauma: clinical examination suggests apophysitis in knee and heel. | ||||||
| a Range of motion (passive) For abbreviations, see Table 3. |
||||||
39 patients were interviewed only, without follow-up invitation: 79% (31/39) scored 48 on OHS, and the remaining 21% (8/39) scored ≥ 44. Among them, patient no. 1 with Ratliff I AVN scored 47 on OHS at 5-year follow-up, despite the fact that on last clinical examination 3 years post-accident, gait was found to be affected, with significant range of motion (ROM) limitations (flexion 80°, internal rotation 5°, external rotation 40°, and abduction 10°) and total collapse of the femoral head. However, during the interview she expressed having hip pain 1–2 times a month with no limitations in daily activities due to impaired hip function. Regardless of this discrepancy between objective findings and subjective view on good outcome, we considered the patient’s outcome as impaired due to her limited ROM, abnormal gait, and radiographic deformity. Patient no. 4 with nonunion scored 48 on OHS at 9-year follow-up and described no symptom/functional deficit (Figure 3). Patient no. 5 with hardware failure following screw fixation of Delbet II fracture scored 48 on OHS at 1-year-follow up. 4 patients with uncomplicated recovery described minor issues during interview: 2 had asymmetric gait (complete subtrochanteric), 1 had mild pain during long-distance running (complete subtrochanteric), and 1 had hip stiffness (Delbet II). 3 patients were dissatisfied with the cosmetic outcome of their treatment because of excessive scar formation.
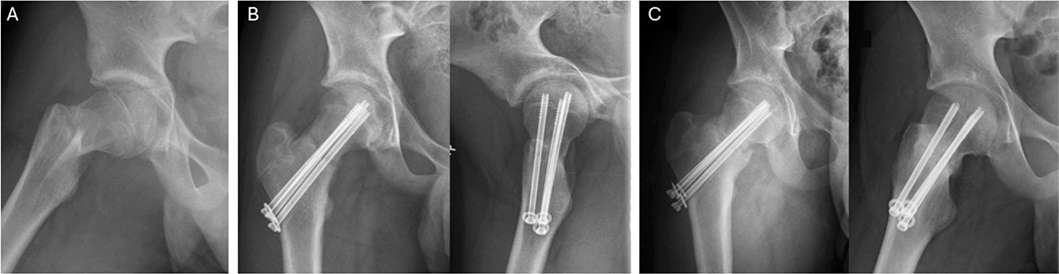
Figure 3. (A) Primary radiograph showing a dislocated Delbet II fracture, (B) fracture alignment following operation, and (C) non-union 7 months post-injury
Discussion
Prior annual incidence of non-pathological proximal femoral fractures has not been reported previously. Our aim was to describe the population-based incidence, complications, and functional outcomes after pediatric proximal femoral fractures in a register-based follow-up study. We found 51 proximal femoral fractures accounting for 2/1,000 pediatric fractures during the study period, with a population-based annual incidence of 1.7/100,000 children. Complications occurred in 16 children, all requiring reoperation. Functional outcomes were satisfactory in 43/46 patients contacted, with impairments found only in patients with AVN.
In contrast to our study, an older Finnish study reported a somewhat higher incidence of 0.6–1/100,000 in < 7-year-old children and 1.5–4/100,00 in 7–16-year-old children, which can be attributed to inclusion of pathological fractures. A Turkish study found a lower incidence of 0.45/100,000 in < 16-year-old children despite inclusion of pathological fractures [20], which may reflect a difference in predisposing factors in different populations. High-energy injury mechanisms such as falls from a height, MVAs, and sports injuries prevailed, which is in line with previous reports [21,22].
Pediatric collum and trochanteric fractures are currently approached in good time, with an emphasis on anatomic reduction and internal fixation, by open reduction, if necessary, to mitigate severe complications such as AVN, coxa vara, and nonunion [4,16,22]. However, a uniform management strategy is yet to be defined. In our study, we encountered a failure of initial nonoperative management of a collum facture, leading to AVN (Figure 4). For us, this emphasizes the importance of internal fixation even in non-displaced femoral collum fractures.
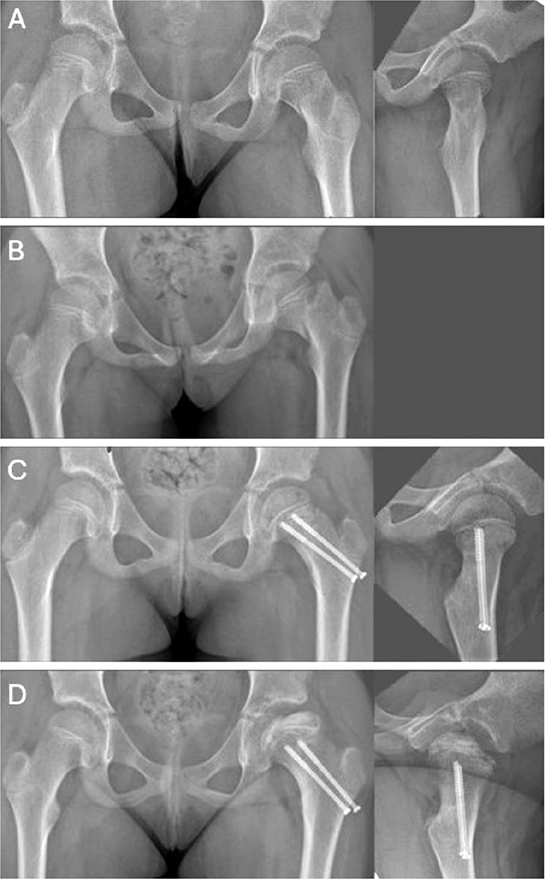
Figure 4. (A) Primary radiographs showing a non-dislocated Delbet II fracture in an 8-year-old girl. (B) Loss of alignment at 10 days’ follow-up. (C) Ratliff type 1 AVN at 3 months post-injury. (D) AVN at 11 months post-injury.
Collum and trochanteric fractures are still complicated by AVN (23%), nonunion (11%), coxa vara (18%), PPC (22%), and LLD (11%) [6]. Our incidences for AVN (15%), non-union (5%), coxa vara (5%), LLD (5%), and PPC (0%) were somewhat lower than previously reported [6]. In addition to small sample size and aggressive operative approach, differences can reflect heterogeneity of complication definitions across studies [6]. While AVN and nonunion are well defined in the pediatric literature [7,16], definitions for coxa vara and LLD were viewed as controversial in our study. We thought complications should be considered as events causing short- or longer-term harm to the child. Coxa vara of > 10°compared with the unaffected side has demonstrated significant difference in Harris Hip Score in 1 study [10], so this definition was chosen. LLD has been defined as a discrepancy of > 1 cm in some studies. We defined LLD as a discrepancy of ≥ 2 cm. In our experience the gait remains unaffected with LLD between 1 and 2 cm, and in the longer term, LLD > 2 cm is often reported as problematic, while the significance of discrepancies below 2 cm is not well established [17].
Definition of complete subtrochanteric fractures of the femur has been versatile in the literature. The latest definition by Pombo and Shilt defined a fracture as subtrochanteric if the fracture line extends to an area that is within 10% of the length of the femur when measured from the lesser trochanter [11]. However, for this study, our patients had subtrochanteric fracture if the fracture line was located entirely within 20% of femoral length as measured from the lesser trochanter, as we view these fractures as different in their fixation nature, with inserting muscles pulling the proximal fragment in flexion, abduction, and external rotation, as opposed to the long oblique fractures of the diaphysis.
The rotational forces of the hip muscles pose a challenge in maintaining closed anatomic reduction of dislocated subtrochanteric fractures, so reduction and fixation is currently opted for [5,8,11]. Our approach reflected this. Complications of complete subtrochanteric fractures include angular deformity (especially varus malunion), nail irritation, and LLD [9]. There is no definition for significant varus/valgus malunion in pediatric subtrochanteric fractures. We used a > 10° definition for varus malunion, a definition used in pediatric femoral shaft fractures, though this is based on general agreement rather than evidence of long-term harm [23]. Flexible intramedullary nails (FIN) have been concluded to be a viable option for school-aged children, but inferior to plating regarding angular deformities [5,9]. Our only varus malunion followed FIN fixation. We noted that the more proximally the subtrochanteric fracture was located, the more likely it was that the surgeon opted for plate fixation, reflecting concerns over FIN stability.
Functional outcomes of collum and trochanteric fractures have mostly been evaluated with criteria set by Ratliff, evaluating pain, movement, activity, and radiographic findings [7]. A meta-analysis including studies between 1960 and 2010 reported good outcomes in 60%, fair in 19%, and poor in 21% of patients, with proximity of the fracture in Delbet classification predicting worse outcomes [6]. Within AVN patients, Ratliff reported worst outcomes with type I AVN (total collapse of femoral head and neck) and more favorable in types II–III (partial collapse) [7]. Outcomes of subtrochanteric fractures have mostly been evaluated with titanium elastic nails (TEN) outcome scoring, which evaluates LLD, malalignment, pain, and complications [8]. These outcomes have mostly been assessed in the context of assessing FIN use or comparing FIN and plate fixation, and reported outcomes have typically been excellent in > 50% of patients [8,9,11].
We used OHS, interviews, and, if needed, clinical examination for outcome assessment in both fracture groups, with an attempt to better reflect patients’ perspective of outcomes, as previously used Ratliff’s and Flynn’s criteria have placed more emphasis on radiographic findings [7,8]. Our OHSs, interview, and clinical examination findings were predominantly very good. We found impaired outcomes only in 3 patients with AVN. This results in a good functional outcome of 83% (15/18) in contacted collum and trochanteric patients, which may reflect our comparably smaller incidence of major complications [6]. Good outcomes applied to 100% (28/28) of contacted subtrochanteric patients.
Limitations
First, a few children might have been treated entirely in the private sector, which may affect the incidence. However, pediatric proximal femoral fractures are almost invariably treated at our tertiary-level university hospital. Second, although we interviewed 46/51 children, we did not invite all to our clinic for an outcome assessment. However, the invitation threshold was low. Our OHSs may reflect a ceiling effect, which is common even among validated PROMs [24]. Acknowledging that OHS is not validated in children or parents as proxies, we included interviews, where patients or parents could express any functional deficit or symptom (that the OHS would not, perhaps, be able to measure). There is no validated pediatric hip PROM in available in Finnish. An English version exists, without recommendation for clinical use [25]. Our good outcomes in 93% (43/46) of contacted patients should be interpreted with caution, as only a subset of patients were invited for clinical examination and radiography, and these conditions carry risk for longer-term morbidity that cannot be assessed in the current study. Coxa vara and LLD have been linked to osteoarthritis [17,26], and long-term effects of varus malunion > 10° are unknown. Finally, injury energy classification was based on subjective judgement.
Conclusion
The incidence of non-pathological pediatric proximal femoral fractures is low. Despite frequent complications, impaired functional outcomes only concerned patients with AVN at a median of 4 years’ follow-up.
- Rockwood C A, Beaty J H, Kasser J R. Rockwood and Wilkins’ fractures in children. 7th ed. Philadelphia: Wolters Kluwer/Lippincott, Williams & Wilkins; 2010, xiii, 1076 p.
- Salonen A, Laitakari E, Berg H E, Felländer-Tsai L, Mattila V M, Huttunen T T. Incidence of femoral fractures in children and adolescents in Finland and Sweden between 1998 and 2016: a binational population-based study. Scand J Surg 2022; 111(1): 14574969221083133. doi: 10.1177/14574969221083133.
- Engström Z, Wolf O, Hailer Y D. Epidemiology of pediatric femur fractures in children: the Swedish Fracture Register. BMC Musculoskelet Disord 2020; 21(1): 796. doi: 10.1186/s12891-020-03796-z.
- Lim E J, Kim B S, Kim M, Shon H C, Kim C H. Open reduction versus closed reduction in internal fixation of displaced femoral neck fracture in children: a systematic review and meta-analysis. J Orthop Surg Res 2023; 18(1): 49. doi: 10.1186/s13018-023-03525-x.
- Zhang Y, Xue Y, Zhao M, Chen X, Gao Q. Titanium elastic nails vs locking plate in pediatric subtrochanteric femur fractures: a systematic review and meta-analysis. Front Pediatr 2023; 11: 1114265. doi: 10.3389/fped.2023.1114265.
- Yeranosian M, Horneff J G, Baldwin K, Hosalkar H S. Factors affecting the outcome of fractures of the femoral neck in children and adolescents: a systematic review. Bone Joint J 2013; 95-B(1): 135-42. doi: 10.1302/0301-620X.95B1.30161.
- Ratliff A H. Fractures of the neck of the femur in children. J Bone Joint Surg Br 1962; 44-B: 528-42. doi: 10.1302/0301-620X.44B3.528.
- Flynn J M, Hresko T, Reynolds R A, Blasier R D, Davidson R, Kasser J. Titanium elastic nails for pediatric femur fractures: a multicenter study of early results with analysis of complications. J Pediatr Orthop 2001; 21(1): 4-8. doi: 10.1097/00004694-200101000-00003.
- Li Y, Heyworth B E, Glotzbecker M, Seeley M, Suppan C A, Gagnier J, et al. Comparison of titanium elastic nail and plate fixation of pediatric subtrochanteric femur fractures. J Pediatr Orthop 2013; 33(3): 232-8. doi: 10.1097/BPO.0b013e318288b496.
- Eberl R, Singer G, Ferlic P, Weinberg A M, Hoellwarth M E. Post-traumatic coxa vara in children following screw fixation of the femoral neck. Acta Orthop 2010; 81(4): 442-5. doi: 10.3109/17453674.2010.501744.
- Pombo M W, Shilt J S. The definition and treatment of pediatric subtrochanteric femur fractures with titanium elastic nails. J Pediatr Orthop 2006; 26(3): 364-70. doi: 10.1097/01.bpo.0000203005.50906.41.
- von Elm E, Altman D G, Egger M, Pocock SJ, Gotzsche P C, Vandenbroucke J P, et al. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. Lancet 2007; 370(9596): 1453-7. doi: 10.1016/S0140-6736(07)61602-X.
- Pakarinen O, Ahonen M, Grahn P, Helenius I, Laaksonen T. Refractures in children. J Bone Joint Surg Am 2025; 107(9): e40. doi: 10.2106/JBJS.24.01014.
- City of Helsinki Executive Office, Urban Research and Statistics. Statistical Yearbook of Helsinki 2019. https://www.hel.fi/hel2/tietokeskus/julkaisut/pdf/20_03_10_Vuosikirjaenglanti2019.pdf [Context Link]. 2014–2023 (accessed 2024, Oct 12).
- Colonna P C. Fracture of the neck of the femur in childhood: a report of six cases. Ann Surg 1928; 88(5): 902-7. doi: 10.1097/00000658-192811000-00012.
- Wang W, Xiong Z, Li Y, Guo Y, Li M, Mei H, et al. Variables influencing radiological fracture healing in children with femoral neck fractures treated surgically: a review of 177 cases. Orthop Traumatol Surg Res 2022; 08(1): 103052. doi: 10.1016/j.otsr.2021.103052.
- Gordon J E, Davis L E. Leg length discrepancy: the natural history (and what do we really know). J Pediatr Orthop 2019; 39 (6, Suppl. 1): S10-S13. doi: 10.1097/BPO.0000000000001396.
- Dawson J, Fitzpatrick R, Carr A, Murray D. Questionnaire on the perceptions of patients about total hip replacement. J Bone Joint Surg Br 1996; 78(2): 185-90.
- Kalairajah Y, Azurza K, Hulme C, Molloy S, Drabu K J. Health outcome measures in the evaluation of total hip arthroplasties: a comparison between the Harris hip score and the Oxford hip score. J Arthroplasty 2005; 20(8): 1037-41. doi: 10.1016/j.arth.2005.04.017.
- Soylemez M S, Bingol I, Yasar N E, Dumlupinar E, Ayvali M O, Ata N, et al. Epidemiology and demographics of pediatric proximal femur fractures in Türkiye: results from a government-based health registry. J Pediatr Orthop B 2024; 33(5): 443-51. doi: 10.1097/BPB.0000000000001127.
- AlKhatib N, Younis M H, Hegazy A, Ibrahim T. Early versus late treatment of paediatric femoral neck fractures: a systematic review and meta-analysis. Int Orthop 2019; 43(3): 677-85. doi: 10.1007/s00264-018-3998-4.
- Togrul E, Bayram H, Gulsen M, Kalaci A, Ozbarlas S. Fractures of the femoral neck in children: long-term follow-up in 62 hip fractures. Injury 2005; 36(1): 123-30. doi: 10.1016/j.injury.2004.04.010.
- Wright J G, Wang E E L, Owen J L, Stephens D, Graham H K, Hanlon M, et al. Treatments for paediatric femoral fractures: a randomised trial. Lancet 2005; 365(9465): 1153-8. doi: 10.1016/S0140-6736(05)71878-X.
- Saarinen A, Pakarinen O, Vaajala M, Liukkonen R, Ponkilainen V, Kuitunen I, et al. Randomized controlled trials reporting patient-reported outcomes with no significant differences between study groups are potentially susceptible to unjustified conclusions: a systematic review. J Clin Epidemiol 2024; 169: 111308. doi: 10.1016/j.jclinepi.2024.111308.
- Saris T F, Kalle J R, Sierevelt I N, Eygendaal D, van Bergen C J. Quality of patient- and proxy-reported outcomes for children with impairment of the lower extremity: a systematic review using the COnsensus-based Standards for selection of health Measurement INstruments methodology. J Child Orthop 2024; 18(1): 96-110. doi: 10.1177/18632521231207081.
- Zhang B, Sun J, Du Y, Shen J, Li T, Zhou Y. Treatment of osteoarthritis secondary to severe coxa vara with modular total hip arthroplasty. Ther Clin Risk Manag 2021; 17: 1199-207. doi: 10.2147/TCRM.S335015.