Uncertainty and risk of misleading conclusions: an umbrella review of the quality of the evidence for ankle arthroscopy
Ville PONKILAINEN 1, Valtteri PANULA 2, Juho LAAKSONEN 2, Anniina LAUREMA 3, Mikko MIETTINEN 4, Ville M MATTILA 1,5,6, and Teemu KARJALAINEN 2
1 Department of Orthopaedics and Traumatology, Tampere University Hospital; 2 Department of Surgery, Central Finland Central Hospital, Jyväskylä; 3 Department of Surgery, Mikkeli Central Hospital, Mikkeli; 4 Department of Orthopaedics and Traumatology, University of Helsinki and Helsinki University Hospital, Helsinki, Uusimaa; 5 COXA Hospital for Joint Replacement, Tampere; 6 Faculty of Medicine and Health Technology, University of Tampere, Tampere, Finland
Background and purpose — Ankle arthroscopy is being increasingly utilized, but its potential benefits and harms remain unclear. This umbrella review aimed to assess the quality of systematic reviews and meta-analyses comparing ankle arthroscopy with equivalent open procedures or nonoperative options.
Methods — A comprehensive search of MEDLINE, Embase, and CENTRAL was conducted on March 22, 2025. 2 reviewers independently screened abstracts and full texts, with conflicts resolved by a third reviewer. Systematic reviews assessing ankle arthroscopy versus any surgery or nonoperative treatment were included. The methodological quality of the reviews was evaluated using AMSTAR 2 criteria, along with an evaluation of whether the GRADE tool was appropriately applied.
Results — The literature search identified 430 studies, of which 29 systematic reviews were included after the screening process. These reviews covered various conditions, including lateral ankle instability, osteoarthritis, fractures, and osteochondral defects. None of the systematic reviews included RCTs comparing arthroscopic procedures with nonoperative treatment. A methodological assessment using AMSTAR 2 criteria identified multiple critical flaws across all reviews, leading to an overall confidence rating of “critically low” for each. 1 study adequately applied the GRADE approach to assess the certainty of the evidence.
Conclusion — The efficacy of ankle arthroscopic procedures remains based solely on observational evidence. Given the critically low methodological quality of existing reviews, conclusions suggesting benefits of ankle arthroscopy, particularly over open procedures, are unreliable and insufficient to inform clinical recommendations. RCTs comparing ankle arthroscopy with nonoperative treatments or sham surgery are urgently needed.
Citation: Acta Orthopaedica 2025; 96: 574–583. DOI: https://doi.org/10.2340/17453674.2025.44330.
Copyright: © 2025 The Author(s). Published by MJS Publishing – Medical Journals Sweden, on behalf of the Nordic Orthopedic Federation. This is an Open Access article distributed under the terms of the Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0/)
Submitted: 2025-04-05. Accepted: 2025-07-02. Published: 2025-07-25.
Correspondence: ville.ponkilainen@tuni.fi
VPo, AL, VM, and TK conceived the study idea. VPo conducted the literature searches. VPa, JL, and VPo screened the articles and extracted the data. VPo wrote the initial draft of the manuscript. All authors reviewed and revised the draft, and approved the final manuscript for publication.
Handling co-editors: Bart A. Swierstra and Robin Christensen
Acta thanks Stig Brorson and Rudolf W Poolman for help with peer review of this manuscript.
Ankle arthroscopy is a widely used technique for diagnosing and treating intra-articular conditions of the ankle joint. The rationale for ankle arthroscopy includes enhanced diagnostic precision and decreased soft-tissue trauma compared with open procedures [1]. Ankle arthroscopy has been used in treating chronic lateral ankle instability, ankle fractures, talar osteochondral defects, ankle osteoarthritis, impingements, removing loose bodies, septic arthritis, arthrofibrosis, and synovitis [2]. It has also been used in reducing joint surface fragments in intra-articular ankle fractures [3]. Multiple literature reviews have advocated the use of ankle arthroscopy and suggested that it is superior or comparable to open procedures in the Broström procedure [4], ankle arthrodesis [5,6], and arthroscopy-assisted ankle fracture surgery [3,7]. However, a recent study identified significant regional variation in its utilization, indicating that either the evidence is not sufficiently reliable to gain widespread acceptance or that robust evidence exists but has not been effectively disseminated [8,9].
To evaluate the efficacy of ankle arthroscopy, systematic reviews and meta-analyses are widely regarded as the main tools also for informing clinical guidelines and treatment recommendations. However, the reliability of a systematic review and meta-analysis depends largely on the quality of the original studies they include, and how the uncertainties of the evidence are reflected in the evidence synthesis. The GRADE approach [10] has highlighted that study design alone is insufficient to determine the certainty of evidence; rather, a structured assessment of risk of bias, inconsistency, imprecision, indirectness, and publication bias is necessary. Any flaws in the synthesis process can lead to biased treatment effect estimates and misleading conclusions. Therefore, for the analysis of ankle arthroscopy, it is crucial to conduct the analyses rigorously as well as communicate the uncertainties of evidence on which treatment decisions are based [10-14]. Concerns over the methodological flaws in orthopedic meta-analyses were raised as early as 2001 [15], and although research quality has generally improved since then, a substantial proportion of studies still exhibit major to extensive methodological shortcomings [16,17], including those published in top orthopedic journals [18].
This umbrella review aimed to evaluate the existing evidence on the efficacy of arthroscopy-assisted ankle procedures and determine whether the systematic reviews informing clinical recommendations are methodologically rigorous and their conclusions are supported by best evidence.
Methods
Study design
We included systematic reviews that followed the PICO framework [19]: Patients: adult patients with any ankle joint condition; Intervention: ankle joint arthroscopic procedures; Comparison: any surgery (including placebo surgery), non-surgical approaches, or open ankle joint procedures; Outcomes: Pain, global improvement, health-related quality of life, participation (return to work or leisure activities), and adverse events. We included all systematic reviews with or without meta-analysis that included observational (non-randomized) and randomized studies meeting the same PICO criteria as the original studies in the umbrella review. Reviews were classified as systematic if the authors explicitly identified them as systematic reviews.
The study was reported in accordance with the PRIOR statement [20].
Search and data extraction
Searches were conducted in the MEDLINE, Embase, and CENTRAL databases on March 22, 2025 (Figure). Search strategies are included in Appendix 1. 2 reviewers independently screened the abstracts and full-text articles, with any conflicts resolved by a third author. Screening was conducted using Covidence software [21]. Additionally, the reference lists of the included articles were screened to identify additional relevant studies.
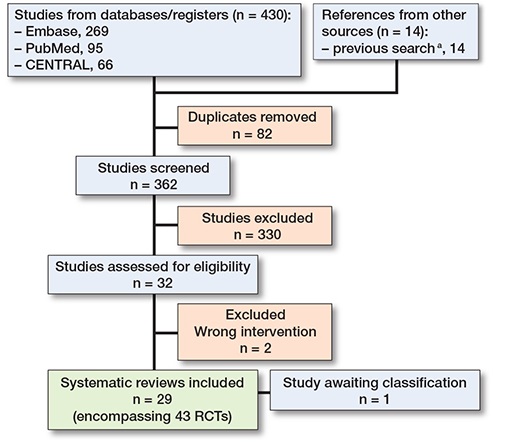
Review process as a flowchart. a Previous search strategy and flowchart is provided in Appendix 3 and 4, see Supplementary data.
Data extraction was performed unblinded by 2 authors: 1 author extracted the data, while a second author reviewed it for inconsistencies. As the aim of this review was to assess the quality of the systematic reviews and whether their conclusions were sound, we did not perform a meta-analysis to quantify treatment effects of procedures. Data was reported using descriptive methods.
The following information was extracted from the studies: characteristics of the intervention and control group, the Risk of Bias (RoB) tool, if certainty of evidence was evaluated with the GRADE tool [10,22], primary outcome(s), primary timepoints, number of included studies, number of included RCTs, review conclusion, clinical recommendation, and the method used to assess the certainty of evidence. The number of included RCTs was confirmed by checking all the original references that the authors labeled as RCTs. In the assessment of certainty of evidence, a study was categorized as “Yes” if the certainty of evidence was evaluated based on the quality of the included studies, meaning that the GRADE approach was applied correctly. The use of GRADE was deemed appropriate when authors assessed the certainty of evidence for each outcome from “High” to “Very Low,” based on the domains of risk of bias, inconsistency, imprecision, indirectness, and publication bias [10]. A study was categorized as “Partially” if the conclusion mentioned that the results were based on retrospective studies or if additional research was deemed necessary. Finally, a study was categorized as “No” if the conclusion did not address these aspects. The assessment was based on the conclusions presented in the abstract and the final conclusions section.
Quality assessment
The methodological quality of the reviews was assessed using A MeaSurement Tool to Assess systematic Reviews II (AMSTAR 2) criteria [23]. AMSTAR 2 was selected over other tools (e.g., ROBIS [24]) because our focus was exclusively on assessing the methodological quality of the included reviews. According to the original AMSTAR 2 publication, items 2, 4, 7, 9, 11, 13, and 15 were identified as critical domains [23]. Reviews were rated based on their methodological quality using 4 categories: High, Moderate, Low, and Critically Low. A review was classified as High quality if it had no or only 1 non-critical weakness, ensuring an accurate and comprehensive summary of the available studies. Moderate quality was assigned to reviews with more than 1 non-critical weakness but no critical flaws, meaning the summary of results was still likely to be accurate. Reviews with 1 critical flaw, regardless of additional non-critical weaknesses, were rated as Low quality, as they might not provide a reliable summary of the available evidence. Finally, reviews with more than 1 critical flaw were considered Critically Low quality, indicating that they should not be relied upon for an accurate and comprehensive synthesis of the studies [23].
Protocol deviations
Initially, the aim of our review was to identify RCTs comparing ankle arthroscopy with placebo or sham surgery or nonoperative treatments. However, as no such RCTs were found, we amended our objective. Specifically, we chose to conduct an umbrella review, qualitatively assessing the quality of existing reviews using the AMSTAR II criteria. Because current guidelines and clinical practices rely heavily on these reviews, we aimed to assess their quality. Given the generally poor quality, the findings of these reviews are not suitable for clinical use. Due to these quality issues, quantitative synthesis is not feasible, as biased primary estimates would lead to biased pooled results. Therefore, we chose to refrain from conducting a post-hoc meta-analysis. This change was made early in the review process, allowing us to adapt our methodology accordingly and provide a broader overview of the current evidence base. These amendments were reported in the PROSPERO registration prospectively (https://www.crd.york.ac.uk/PROSPERO/view/CRD42024618073).
Ethics, registration, funding, and disclosures
This work is a systematic review of published studies; no primary human or animal research was conducted. Therefore, institutional review board approval was not required. This systematic review was prospectively registered in PROSPERO: CRD42024618073 [25]. This research received no external funding. The datasets generated and analyzed during this study are available from the corresponding author upon request. The authors declare that they have no competing interests. Complete disclosure of interest forms according to ICMJE are available on the article page, doi: 10.2340/17453674.2025.44330
Results
The literature search identified 430 studies (see Figure). After excluding 68 duplicates, title and abstract screening was conducted for 362 studies, resulting in 32 articles to full-text phase. Following full-text review, 30 studies were included, and 2 studies were excluded due to not fulfilling the inclusion criteria and 1 study [23] was classified as “awaiting classification,” as it was an abstract of a study that was not published (Appendix 2). 29 systematic reviews were included in this umbrella review, encompassing 457 original publications, of which 43 (9%) were RCTs [2-7,27-49].
The included studies investigated the effect of ankle arthroscopy for various conditions: lateral ankle instability (n = 13), ankle osteoarthritis (n = 6), ankle fractures (n = 6), osteochondral defects (n = 3). 1 review encompassed numerous indications, including all previously noted conditions as well as impingement, loose bodies, septic arthritis, arthrofibrosis, and synovitis [2]. In the included studies, meta-analysis was conducted in 19 of them. None of the systematic reviews included RCTs that compared ankle arthroscopy with nonoperative treatment, placebo, or sham surgery. None of the included reviews prespecified their primary timepoints.
Arthroscopic reconstruction for ankle instability
14 systematic reviews investigated the effect of arthroscopic surgery for lateral ankle instability [2,4,42,30,32,36,38,39,41,42,45-49] comparing arthroscopic and open lateral ankle ligament repair procedures in an adult population. 10 reviews performed meta-analysis. The reviews were published between 2015 and 2024. They included a median of 8 (range 4–44) studies and median of 420 (range 207–2,041) patients. 9 reviews included RCTs, yet none of the reviews performed analyses using only RCTs. The primary outcomes were patient-reported outcome measures (PROMs) in all studies.
7 of the reviews did not assess the risk of bias of the included studies, while 4 used the RoB I or II tool. None of the studies employed the GRADE approach to assess the certainty of the evidence. Overall confidence rating based on AMSTAR 2 criteria was Critically Low for all reviews (flaws in 6–16 out of 16 criteria) assessing arthroscopic surgery for lateral ankle instability (Table 1). Flaws were present in 5–7 out of 7 critical items.
| Study | Items (see below) | |||||||||||||||
| 1 | 2a | 3 | 4a | 5 | 6 | 7a | 8 | 9 a | 10 | 11a | 12 | 13a | 14 | 15a | 16 | |
| Arthroscopic reconstruction for ankle instability | ||||||||||||||||
| Attia 2021 [4] | Yes | No | No | Partial | Yes | No | No | Partial | Partial | No | No | No | No | No | Yes | No |
| Alhaddad 2023 [41] | Yes | Partial | No | Partial | Yes | Yes | No | Yes | Partial | No | – | – | No | No | – | Yes |
| Brown 2018 [38] | No | No | No | Partial | Yes | Yes | No | Partial | No | No | – | – | No | No | – | Yes |
| Brown 2020 [42] | Yes | No | No | Partial | Yes | Yes | No | Partial | No | No | No | No | No | No | No | Yes |
| Guelfi 2016 [36] | Yes | No | No | No | Yes | No | No | Partial | No | No | No | No | No | Yes | No | Yes |
| Matsui 2016 [30] | No | No | No | Partial | No | No | No | No | No | No | – | – | No | No | No | Yes |
| Moorthy 2021 [32] | Yes | Partial | Yes | Partial | Yes | Yes | No | Partial | Partial | No | Yes | Yes | No | Yes | Yes | Yes |
| Song 2018 [39] | Yes | Partial | Yes | Partial | Yes | Yes | No | Yes | Partial | No | Yes | Yes | Yes | Yes | No | Yes |
| Tonsuthanluck 2024 [45] | Yes | Partial | Yes | Partial | Yes | Yes | No | Partial | Partial | No | No | No | No | No | No | Yes |
| Wang 2024 [46] | Yes | No | No | Partial | Yes | Yes | No | Partial | No | No | No | No | No | Yes | Yes | Yes |
| Wittig 2022 [47] | Yes | No | Yes | Partial | No | No | No | Yes | No | No | No | No | No | Yes | No | Yes |
| Zhao 2023 [48] | Yes | Partial | Yes | Partial | Yes | Yes | No | Yes | Partial | No | Yes | Yes | Yes | Yes | No | Yes |
| Zhi 2020 [49] | Yes | Partial | Yes | Partial | Yes | Yes | No | Yes | Partial | No | Yes | No | No | No | No | Yes |
| Arthroscopic-assisted fusion for ankle osteoarthritis | ||||||||||||||||
| Bai 2021 [5] | Yes | Partial | No | Partial | Yes | Yes | No | Partial | Partial | No | Yes | No | No | No | Yes | Yes |
| Honnenahalli 2017 [37] | Yes | Partial | Yes | Partial | Yes | Yes | No | Yes | Partial | No | Yes | No | Yes | Yes | Yes | Yes |
| Lorente 2023 [43] | Yes | Partial | Yes | Partial | Yes | Yes | Yes | Partial | Partial | No | Yes | Yes | Yes | Yes | Yes | Yes |
| Mok 2020 [31] | Yes | Partial | No | Partial | Yes | Yes | No | Yes | Partial | No | Yes | Yes | Yes | Yes | Yes | Yes |
| Park 2018 [40] | Yes | No | No | Partial | Yes | Yes | No | Yes | No | No | – | – | No | Yes | – | Yes |
| Xing 2023 [6] | Yes | Partial | No | Partial | No | No | No | Partial | Partial | No | No | No | Yes | No | Yes | Yes |
| Arthroscopic-assisted reduction for ankle fractures | ||||||||||||||||
| Chen 2015 [27] | No | No | No | No | Yes | Yes | No | Partial | No | No | – | – | No | No | – | Yes |
| Gonzalez 2016 [7] | No | No | No | No | No | No | No | No | No | No | – | – | No | No | – | Yes |
| Lee 2017 [3] | Yes | Partial | No | Partial | Yes | Yes | No | Partial | Partial | No | No | No | No | No | Yes | Yes |
| Meyer-Pries 2025 [44] | Yes | Partial | Yes | Partial | Yes | Yes | No | Partial | Partial | No | No | No | No | Yes | No | Yes |
| Zhang 2023 [34] | Yes | Partial | No | Partial | Yes | No | No | Partial | Partial | No | Yes | Yes | Yes | No | Yes | Yes |
| Zhuang 2023 [35] | Yes | Partial | No | Partial | Yes | Yes | No | Partial | Partial | No | Yes | No | No | Yes | Yes | No |
| Debridement or autologous chondrocyte implantation for osteochondral lesions | ||||||||||||||||
| Erickson 2018 [28] | Yes | No | No | Partial | Yes | Yes | No | No | No | No | – | – | No | No | – | Yes |
| Marin Fermin 2021 [29] | No | Partial | No | Partial | Yes | Yes | Yes | No | Partial | No | – | – | No | No | – | Yes |
| Zengerink 2010 [33] | No | No | No | Partial | Yes | No | No | No | Partial | No | – | – | No | No | – | No |
| Multiple indications | ||||||||||||||||
| Glazebrook 2009 [2] | No | No | No | No | Yes | No | No | No | No | No | – | – | No | No | – | No |
| Item 1 | Did the research questions and inclusion criteria for the review include the components of PICO? | |||||||||||||||
| Item 2 | Did the report of the review contain an explicit statement that the review methods were established prior to the conduct of the review and did the report justify any significant deviations from the protocol? | |||||||||||||||
| Item 3 | Did the review authors explain their selection of the study designs for inclusion in the review? | |||||||||||||||
| Item 4 | Did the review authors use a comprehensive literature search strategy? | |||||||||||||||
| Item 5 | Did the review authors perform study selection in duplicate? | |||||||||||||||
| Item 6 | Did the review authors perform data extraction in duplicate? | |||||||||||||||
| Item 7 | Did the review authors provide a list of excluded studies and justify the exclusions? | |||||||||||||||
| Item 8 | Did the review authors describe the included studies in adequate detail? | |||||||||||||||
| Item 9 | Did the review authors use a satisfactory technique for assessing the risk of bias (RoB) in individual studies that were included in the review? | |||||||||||||||
| Item 10 | Did the review authors report on the sources of funding for the studies included in the review? | |||||||||||||||
| Item 11 | If meta-analysis was performed, did the review authors use appropriate methods for statistical combination of results? | |||||||||||||||
| Item 12 | If meta-analysis was performed, did the review authors assess the potential impact of RoB in individual studies on the results of the meta-analysis or other evidence synthesis? | |||||||||||||||
| Item 13 | Did the review authors account for RoB in primary studies when interpreting/discussing the results of the review? | |||||||||||||||
| Item 14 | Did the review authors provide a satisfactory explanation for, and discussion of, any heterogeneity observed in the results of the review? | |||||||||||||||
| Item 15 | If they performed quantitative synthesis, did the review authors carry out an adequate investigation of publication bias (small study bias) and discuss its likely impact on the results of the review? | |||||||||||||||
| Item 16 | Did the review authors report any potential sources of conflict of interest, including any funding they received for conducting the review? | |||||||||||||||
| “–”: No meta-analysis conducted | ||||||||||||||||
| a AMSTAR 2 critical domains. | ||||||||||||||||
4 reviews concluded that arthroscopic surgery is as good as open surgery [32,36,46,48], while 10 reviews concluded it is superior to open surgery [2,4,30,38,39,41,42,45,47,49], none acknowledging that the evidence was by and large drawn from observational studies and none performed analysis based on RCTs (Table 2). 1 review [36] claimed excellent efficacy despite none of the included studies directly assessing the procedure’s efficacy.
Arthroscopic-assisted fusion for ankle osteoarthritis
7 reviews investigated the effect of arthroscopic surgery for ankle osteoarthritis [2,5,6,31,37,40,43] comparing arthroscopic and open ankle arthrodesis in adult population. 5 reviews performed meta-analysis. The reviews were published between 2015 and 2023. They included a median of 10 studies (range 6–18) and median of 487 (range 286–1,102) patients. 1 of the reviews found 15 RCTs [5], while none of the other reviews found any RCTs. After reviewing the included studies, we found that 8 of the references could not be found from PubMed or Google Scholar (Li 2017, Shi 2018a, Shi 2018b, Zhu 2018, Wang 2018, Li 2018a, Li 2018b, Liu 2018), 6 studies were clearly reported as retrospective studies (Meng 2013, Nielsen 2008, Peterson 2010, Townshend 2013, Quayle 2018, Woo 2019), and 1 was stated to be an RCT (Hou 2017), but the full-text version of the article was not found [5]. The primary outcomes varied across all the meta-analyses, including fusion rate, complication rate, and PROMs. None of the studies specified predetermined primary time points.
2 of the reviews did not assess the risk of bias in the included studies, while 1 study used the RoB I tool, 1 used the RoB II tool, and 3 studies applied the Newcastle–Ottawa Scale (NOS) for observational studies. 1 study applied the GRADE approach appropriately and drew conclusions per outcome based on the certainty of evidence [43]. 1 of the studies mentioned using the GRADE approach to assess the certainty of the evidence but the reporting was not transparent and it is unclear which factors impacted the certainty ratings [5]. Certainty was reported as a single paragraph mentioning that the certainty was either “medium” (rather than “moderate,” as defined by GRADE) or “low.” The most common reasons for downgrading were “unclear random method” and “calculation of the optimal sample size.” However, these factors alone are not reasons for downgrading the certainty level. No additional reasons were provided, making the application of the GRADE approach non-reproducible. The overall confidence based on the AMSTAR 2 criteria was Critically Low (flaws in 5–16 out of 16) (see Table 1). Flaws were present in 4–7 out of 7 critical items.
All reviews concluded that arthroscopic-assisted surgery was superior to open surgery, none acknowledging that the evidence was drawn from observational studies and none performed analysis based on RCTs (see Table 2). 1 study found that arthroscopic-assisted surgery is associated with higher complication rates, yet still concluded that the surgeons should have “good arthroscopic skills” when performing these procedures [41].
Arthroscopic-assisted reduction for ankle fractures
7 reviews investigated the effect of arthroscopic surgery for ankle fractures [2,3,7,27,34,35,44], all comparing arthroscopy-assisted and open reduction and internal fixation for ankle fractures. 4 of the reviews performed meta-analysis. The reviews were published between 2015 and 2025. They included a median of 10 (range 4–18) studies and median of 597 (range 188–861) patients. 5 reviews included RCTs, of which none included only RCTs. The primary outcomes were PROMs in all studies.
2 of the reviews did not assess the risk of bias in the included studies, while 2 studies used the RoB II and 1 ROB I tools, 1 applied NOS for observational studies, and 1 used modified Coleman Methodology Score (CMS). None of the studies employed the GRADE approach to assess the certainty of the evidence.
The overall confidence based on the AMSTAR 2 criteria was Critically Low (flaws in 9–16 out of 16) for all reviews (see Table 1). Flaws were present in 5–7 out of 7 critical items.
The conclusions varied between arthroscopic-assisted surgery being superior and comparable to open surgery, none acknowledging that the evidence was drawn from observational studies and none performed analysis based on RCTs (see Table 2).
Debridement or autologous chondrocyte implantation for osteochondral lesions
4 reviews investigated the effect of arthroscopic surgery for osteochondral defects including different interventions, such as debridement only, debridement and drilling, debridement and curettage, microfractures, internal fixation of the loose bodies, and arthroscopic matrix induced autologous chondrocyte implantation (MACI) [2,28,29,33]. None of the reviews performed meta-analysis. The reviews were published between 2015 and 2021. They included a median of 19 (range 4–52) studies and median of 343 (range 189–1,361) patients. 3 reviews included RCTs, of which none included only RCTs. The primary outcomes were PROMs in all studies.
1 of the reviews did not assess the risk of bias in the included studies, while 1 study used the NOS, 1 the modified CMS, and 1 applied the ROBIS tool. None of the studies employed the GRADE approach to assess the certainty of the evidence.
The overall confidence, based on the AMSTAR 2 criteria, was Critically Low for all included reviews (flaws in 12–16 out of 16). Flaws were present in 6–7 out of 7 critical items.
The conclusions were generally cautious, with no review asserting the efficacy of any surgical approach and most stating that the available evidence is insufficient to support 1 type of surgery over another, none acknowledging that the evidence was drawn from observational studies and none performed analysis based on RCTs (see Table 2).
AMSTAR 2 criteria
Included reviews revealed several critical flaws in review methods, as assessed by the AMSTAR 2 criteria (see Table 1). The most common issues were related to assessing study protocol (item 2), search strategy (item 4), and risk of bias assessment (item 9), none of which were conducted properly in any of the studies. Among these, items 2, 4, and 9 are classified as critical items according to the AMSTAR 2 criteria. Additionally, 27 studies did not specify reasons for excluding studies (Item 7) and 20 did not specify reasons for included non-randomized studies (Item 3). At best, 1 of the reviews met up to 11 out of 16 of the AMSTAR 2 criteria [43].
Discussion
In this umbrella review of systematic reviews on ankle arthroscopy, we found no evidence supporting the efficacy of ankle arthroscopic surgery in chronic lateral ankle instability, ankle fractures, talar osteochondral defects, ankle osteoarthritis, impingements, removing loose bodies, septic arthritis, arthrofibrosis, or synovitis. Specifically, no studies compared arthroscopic surgery with placebo or no treatment, nor did we identify evidence demonstrating its superiority over nonoperative management. Consequently, the perceived efficacy of these procedures is primarily based on post-surgical improvements, which does not establish causality—patients may improve despite, rather than because of, surgery. Therefore, no causal conclusions can be drawn from the existing body of literature and further reviews based on the same methodologically flawed primary data will constitute a waste of research. Furthermore, the quality of systematic reviews concluding benefits of arthroscopic surgery over open procedures was poor: methods were inadequate or transparency lacking, and conclusions rarely reflected the uncertainties in the available evidence.
Treatment practices in modern medicine rely on data from high-quality RCTs, which can be synthesized in meta-analyses that provide a comprehensive evaluation of both benefits and harms. A well-conducted interventional systematic review and meta-analysis should go beyond pooling data; it must also assess the certainty of the best available estimates of treatment effect and communicate shortcomings of the evidence clearly in the conclusion [10,22]. None of the reviews in the present study managed to account for all factors that impact the certainty of evidence, and most failed on multiple aspects [12].
Conclusions from systematic reviews need to be rigorous because they typically contribute to the treatment guidelines [22]. Including data from flawed studies is not necessarily a critical problem per se if the conclusions reflect the uncertainties and the review highlights the current key evidence gaps to guide future research. The problem arises when firm and biased conclusions are drawn based on biased data. This can mislead readers and steer guidelines in the wrong direction, potentially causing harm to patients, and was often found in our study [11].
Most of the included reviews supported the use of ankle arthroscopy, despite the absence of studies directly comparing it with nonoperative treatment. These selectively interpreted conclusions highlight a second concerning practice referred to as spin [50,51]. Even when the data does not demonstrate any benefits over no surgery, or the benefits are clearly negligible compared with open procedures, the reviews may still claim benefits for arthroscopy. This problem has been recognized outside these reviews [50-57], and is commonly observed in orthopedic research as well [58-60]. The presence of spin can be either intentional or unintentional, driven by factors such as funding-related reasons or the need to enhance the manuscript’s likelihood of publication [60].
Our study revealed first that greater efforts should be made to compare the benefits of ankle arthroscopy against placebo or nonoperative controls through randomized controlled trials, as this is the only reliable way to evaluate the true effect of any intervention. Second, systematic reviews and meta-analyses should adhere to established guidelines such as PRISMA and apply the GRADE approach when synthesizing evidence [10,14,61]. This would enhance methodological quality and lead to more robust conclusions, thereby improving their suitability for clinical decision-making. Third, journal editors and peer reviewers should require transparent reporting and ensure that conclusions accurately reflect the uncertainty of the underlying evidence.
Strengths
We used a systematic and transparent approach to evaluate and report methodological issues across the included studies. The umbrella review design offers a unique advantage by providing a comprehensive synthesis of evidence from multiple systematic reviews, particularly those commonly used to inform clinical decision-making. Such a broad, high-level perspective is not achievable with traditional review designs. Additionally, the review protocol was prospectively registered, and any deviations from the original plan were clearly documented and updated in the registry to ensure transparency.
Limitations
Due to non-transparent reporting of the included studies, we were sometimes unable to assess whether proper methods were used or to explain how studies arrived at the conclusions they did. As an umbrella review, this study was not aimed at estimating the effects of studied interventions but rather at summarizing evidence at a higher level than RCTs, whether reviews are reliable for clinical guidelines, and to identify key evidence gaps.
Conclusions
The efficacy of ankle arthroscopic procedures remains based solely on observational evidence. Given the critically low methodological quality of existing reviews, conclusions suggesting benefits of ankle arthroscopy, particularly over open procedures, are unreliable and insufficient to inform clinical recommendations. RCTs comparing ankle arthroscopy with nonoperative treatments or sham surgery are urgently needed.
In perspective, to advance the field, we propose that: (i) greater efforts be made to compare the benefits of ankle arthroscopy against placebo or nonoperative controls with RCT; (ii) systematic reviews and meta-analyses adhere to established guidelines (PRISMA) and apply the GRADE approach to synthesize the evidence. Furthermore, journals should require transparent reporting and ensure that conclusions appropriately reflect the uncertainty of the evidence.
Supplementary data
Appendices 1–4 are available as supplementary data on the article page, doi: 10.2340/17453674.2025.44330
- Pritsch M, Horoshovski H, Farine I. Ankle arthroscopy. Clin Orthop Relat Res 1984; (184):: 137-40.
- Glazebrook M A, Ganapathy V, Bridge M A, Stone J W, Allard J-P. Evidence-based indications for ankle arthroscopy. Arthroscopy 2009; 25: 1478-90. doi: 10.1016/j.arthro.2009.05.001.
- Lee K M, Ahmed S, Park M S, Sung K H, Lee S Y, Koo S. Effectiveness of arthroscopically assisted surgery for ankle fractures: a meta-analysis. Injury 2017; 48: 2318-22. doi: 10.1016/j.injury.2017.07.011.
- Attia A K, Taha T, Mahmoud K, Hunt K J, Labib S A, d’Hooghe P. Outcomes of open versus arthroscopic Broström surgery for chronic lateral ankle instability: a systematic review and meta-analysis of comparative studies. Orthop J Sports Med 2021; 9: 23259671211015207. doi: 10.1177/23259671211015207.
- Bai Z, Yang Y, Chen S, Dong Y, Cao X, Qin W, et al. Clinical effectiveness of arthroscopic vs open ankle arthrodesis for advanced ankle arthritis: a systematic review and meta-analysis. Medicine 2021; 100: e24998. doi: 10.1097/MD.0000000000024998.
- Xing G, Xu M, Yin J, Wei Y, Zhang L. Effectiveness of arthroscopically assisted surgery for ankle arthrodesis. J Foot Ankle Surg 2023; 62: 398-404. doi: 10.1053/j.jfas.2022.12.001.
- Gonzalez T A, Macaulay A A, Ehrlichman L K, Drummond R, Mittal V, DiGiovanni C W. Arthroscopically assisted versus standard open reduction and internal fixation techniques for the acute ankle fracture. Foot Ankle Int 2016; 37: 554-62. doi: 10.1177/1071100715620455.
- Ponkilainen V, Laurema A, Mattila V M, Karjalainen T. Regional variation in low-value musculoskeletal surgery: a nationwide study from the Finnish Care Register. Acta Orthop 2024; 95: 553. doi: 10.2340/17453674.2024.41930.
- Ponkilainen V, Laurema A, Mattila V M, Karjalainen T. Response to Letter: Regional variation in low-value musculoskeletal surgery: a nationwide study from the Finnish Care Register. Acta Orthop 2024; 95: 748-9. doi: 10.2340/17453674.2024.42635.
- Guyatt G H, Oxman A D, Vist G E, Kunz R, Falck-Ytter Y, Alonso-Coello P, et al. GRADE: an emerging consensus on rating quality of evidence and strength of recommendations. BMJ 2008; 336: 924-6. doi: 10.1136/bmj.39489.470347.AD.
- Foroutan F, Guyatt G, Alba A C, Ross H. Meta-analysis: mistake or milestone in medicine? Heart 2018; 104: 1559-61. doi: 10.1136/heartjnl-2018-313042.
- Cumpston M, Li T, Page M J, Chandler J, Welch V A, Higgins J P, et al. Updated guidance for trusted systematic reviews: a new edition of the Cochrane Handbook for Systematic Reviews of Interventions. Cochrane Database Syst Rev 2019; 10.1002/14651858.ED000142. doi: 10.1002/14651858.ED000142.
- Vetter T R. Systematic review and meta-analysis: sometimes bigger is indeed better. Anesth Analg 2019; 128: 575-83. doi: 10.1213/ANE.0000000000004014.
- Guyatt G, Hultcrantz M, Agoritsas T, Iorio A, Vandvik P O, Montori V M. Why Core GRADE is needed: introduction to a new series in the BMJ. BMJ 2025; 389: e081902. doi: 10.1136/bmj-2024-081902.
- Bhandari M, Morrow F, Kulkarni A V, Tornetta P, III. Meta-analyses in orthopaedic surgery: a systematic review of their methodologies. J Bone Joint Surg Am 2001; 83: 15-24. PMID: 11205853
- Dijkman B G, Abouali J A K, Kooistra B W, Conter H J, Poolman R W, Kulkarni A V, et al. Twenty years of meta-analyses in orthopaedic surgery: has quality kept up with quantity? J Bone Joint Surg Am 2010; 92: 48-57. doi: 10.2106/JBJS.I.00251.
- Simunovic N, Sprague S, Bhandari M. Methodological issues in systematic reviews and meta-analyses of observational studies in orthopaedic research. J Bone Joint Surg Am 2009; 91: 87-94. doi: 10.2106/jbjs.H.01576.
- Gagnier J J, Kellam P J. Reporting and methodological quality of systematic reviews in the orthopaedic literature. J Bone Joint Surg Am 2013; 95: e77. doi: 10.2106/jbjs.L.00597.
- Schardt C, Adams M B, Owens T, Keitz S, Fontelo P. Utilization of the PICO framework to improve searching PubMed for clinical questions. BMC Med Inform Decis Mak 2007; 7: 1-6. doi: 10.1186/1472-6947-7-16.
- Gates M, Gates A, Pieper D, Fernandes R M, Tricco A C, Moher D, et al. Reporting guideline for overviews of reviews of healthcare interventions: development of the PRIOR statement. BMJ 2022; 378. doi: 10.1136/bmj-2022-070849.
- Covidence systematic review software. Melbourne, Australia: Veritas Health Innovation.
- Guyatt G H, Oxman A D, Kunz R, Vist G E, Falck-Ytter Y, Schünemann H J. What is “quality of evidence” and why is it important to clinicians? BMJ 2008; 336: 995-8. doi: 10.1136/bmj.39490.551019.BE.
- Shea B J, Reeves B C, Wells G, Thuku M, Hamel C, Moran J, et al. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ 2017; 358: j4008. doi: 10.1136/bmj.j4008.
- Whiting P, Savović J, Higgins J P, Caldwell D M, Reeves B C, Shea B, et al. ROBIS: a new tool to assess risk of bias in systematic reviews was developed. J Clin Epidemiol 2016; 69: 225-34. doi: 10.1016/j.jclinepi.2015.06.005.
- Ponkilainen V, Karjalainen T, Laurema A. PROSPERO registration; Effect of ankle arthroscopy: umbrella review. 2024. https://www.crd.york.ac.uk/PROSPERO/view/CRD42024618073
- Tornberg H, Hartman H C, Fine-Lease P, Gianakos A. Podium Presentation Title: Arthroscopic management of talus fracture: a review of the clinical outcomes and surgical technique. Arthroscopy 2025; 41: e17-e18.
- §Chen X Z, Chen Y, Liu C G, Yang H, Xu X D, Lin P. Arthroscopy-assisted surgery for acute ankle fractures: a systematic review. Arthroscopy 2015; 31: 2224-31. doi: 10.1016/j.arthro.2015.03.043.
- Erickson B, Fillingham Y, Hellman M, Parekh S G, Gross C E. Surgical management of large talar osteochondral defects using autologous chondrocyte implantation. Foot Ankle Surg 2018; 24: 131-6. doi: 10.1016/j.fas.2017.01.002.
- Marín Fermín T, Hovsepian J M, D’Hooghe P, Papakostas E T. Arthroscopic debridement of osteochondral lesions of the talus: a systematic review. Foot 2021; 49: 101852. doi: 10.1016/j.foot.2021.101852.
- Matsui K, Burgesson B, Takao M, Stone J, Guillo S, Glazebrook M, et al. Minimally invasive surgical treatment for chronic ankle instability: a systematic review. Knee Surg Sports Traumatol Arthrosc 2016; 24: 1040-8. doi: 10.1007/s00167-016-4041-1.
- Mok T N, He Q, Panneerselavam S, Wang H, Hou H, Zheng X, et al. Open versus arthroscopic ankle arthrodesis: a systematic review and meta-analysis. J Orthop Surg Res 2020; 15: 187. doi: 10.1186/s13018-020-01708-4.
- Moorthy V, Sayampanathan A A, Yeo N E M, Tay K S. Clinical outcomes of open versus arthroscopic Broström procedure for lateral ankle instability: a meta-analysis. J Foot Ankle Surg 2021; 60: 577-54. doi: 10.1053/j.jfas.2020.10.001.
- Zengerink M, Struijs P A A, Tol J L, van Dijk C N. Treatment of osteochondral lesions of the talus: a systematic review. Knee Surg Sports Traumatol Arthrosc 2010; 18: 238-46. doi: 10.1007/s00167-009-0942-6.
- Zhang G, Chen N, Ji L, Sun C, Ding S-L. Arthroscopically assisted versus open reduction internal fixation for ankle fractures: a systematic review and meta-analysis. J Orthop Surg Res 2023; 18: 118. doi: 10.1186/s13018-023-03597-9.
- Zhuang C, Guo W, Chen W, Pan Y, Zhuang R. Arthroscopically assisted internal fixation for treatment of acute ankle fracture: a systematic review and meta-analysis of comparative studies. PLoS One 2023; 18: e0289554. doi: 10.1371/journal.pone.0289554.
- Guelfi M, Zamperetti M, Pantalone A, Usuelli F G, Salini V, Oliva X M. Open and arthroscopic lateral ligament repair for treatment of chronic ankle instability: a systematic review. Foot Ankle Surg 2018; 24: 11-18. doi: 10.1016/j.fas.2016.05.315.
- Honnenahalli Chandrappa M, Hajibandeh S, Hajibandeh S. Ankle arthrodesis—open versus arthroscopic: a systematic review and meta-analysis. J Clin Orthop Trauma 2017; 8: S71-S77. doi: 10.1016/j.jcot.2017.03.010.
- Brown A J, Shimozono Y, Hurley E T, Kennedy J G. Arthroscopic repair of lateral ankle ligament for chronic lateral ankle instability: a systematic review. Arthroscopy 2018; 34: 2497-503. doi: 10.1016/j.arthro.2018.02.034.
- Song Y-J, Hua Y-H. Similar outcomes at early term after arthroscopic or open repair of chronic ankle instability: a systematic review and meta-analysis. J Foot Ankle Surg 2019; 58: 312-19. doi: 10.1053/j.jfas.2018.08.026.
- Park J H, Kim H J, Suh D H, Lee J W, Kim H J, Oh M J, et al. Arthroscopic versus open ankle arthrodesis: a systematic review. Arthroscopy 2018; 34: 988-97. doi: 10.1016/j.arthro.2017.08.284.
- Alhaddad A, Gronfula A G, Alsharif T H, Khawjah A, Al Shareef N S, AlThagafi A A, et al. A comparative analysis of complication rates in arthroscopic repair of the lateral ankle ligament and the Brostrom-Gould technique: a systematic review. Cureus 2023; 15. doi: 10.7759/cureus.48460.
- Brown A J, Shimozono Y, Hurley E T, Kennedy J G. Arthroscopic versus open repair of lateral ankle ligament for chronic lateral ankle instability: a meta–analysis. Knee Surg Sports Traumatol Arthrosc 2020; 28: 1611-18. doi: 10.1007/s00167-018-5100-6,
- Lorente A, Pelaz L, Palacios P, Bautista I J, Mariscal G, Barrios C, et al. Arthroscopic vs. open-ankle arthrodesis on fusion rate in ankle osteoarthritis patients: a systematic review and meta-analysis. J Clin Med 2023; 12: 3574. doi: 10.3390/jcm12103574.
- Meyer-Pries M, Hajymiri M, Lytras T, Manolopoulos P, Ntourakis D. Arthroscopy-assisted open reduction internal fixation versus conventional open reduction internal fixation in the treatment of ankle fractures: a systematic review with meta-analysis. HSS J 2023; 21(1): 86-92. doi: 10.1177/15563316231204616.
- Tonsuthanluck S, Handoyo H R, Tharincharoen R, Angthong C. Comparative analyses of arthroscopic and open repairs of lateral ligament complex injuries of the ankle: a systematic review and meta-analysis of the medium-term outcomes. Eur J Orthop Surg Traumatol 2024; 34: 1487-95. doi: 10.1007/s00590-023-03825-2.
- Wang D, Yuan J, Wu Y. Efficacy and complication of keyhole surgery and open surgery for repairing fibular collateral ligament in the persistent lateral ankle joint instability treatment: a protocol for systematic review and meta analysis. Medicine 2024; 103: e39656. doi: 10.1097/MD.0000000000039656.
- Wittig U, Hohenberger G, Ornig M, Schuh R, Leithner A, Holweg P. All-arthroscopic reconstruction of the anterior talofibular ligament is comparable to open reconstruction: a systematic review. EFORT Open Rev 2022; 7: 3-12. doi: 10.1530/EOR-21-0075.
- Zhao B, Sun Q, Xu X, Liu Y, Zhao Y, Gao Y, et al. Comparison of arthroscopic and open Brostrom-Gould surgery for chronic ankle instability: a systematic review and meta-analysis. J Orthop Surg Res 2023; 18: 866. doi: 10.1186/s13018-023-04292-5.
- §Zhi X, Lv Z, Zhang C, Kong C, Wei S, Xu F. Does arthroscopic repair show superiority over open repair of lateral ankle ligament for chronic lateral ankle instability: a systematic review and meta-analysis. J Orthop Surg Res 2020; 15: 1-12. doi: 10.1186/s13018-020-01886-1.
- Boutron I, Dutton S, Ravaud P, Altman D G. Reporting and interpretation of randomized controlled trials with statistically nonsignificant results for primary outcomes. JAMA 2010; 303: 2058-64. doi: 10.1001/jama.2010.651.
- Yavchitz A, Boutron I, Bafeta A, Marroun I, Charles P, Mantz J, et al. Misrepresentation of randomized controlled trials in press releases and news coverage: a cohort study. PLos Med 2012; 9(9):e1001308. doi: 10.1371/journal.pmed.1001308.
- Hewitt C E, Mitchell N, Torgerson D J. Listen to the data when results are not significant. BMJ 2008; 336: 23-5. doi: 10.1136/bmj.39379.359560.AD.
- Boutron I, Altman D G, Hopewell S, Vera-Badillo F, Tannock I, Ravaud P. Impact of spin in the abstracts of articles reporting results of randomized controlled trials in the field of cancer: the SPIIN randomized controlled trial. J Clin Oncol 2014; 32: 4120-26. doi: 10.1200/JCO.2014.56.7503.
- Mathieu S, Boutron I, Moher D, Altman D G, Ravaud P. Comparison of registered and published primary outcomes in randomized controlled trials. JAMA 2009; 302: 977-84. doi: 10.1001/jama.2009.1242.
- Le Henanff A, Giraudeau B, Baron G, Ravaud P. Quality of reporting of noninferiority and equivalence randomized trials. JAMA 2006; 295: 1147-51. doi: 10.1001/jama.295.10.1147.
- Premji S, Messing K, Lippel K. Would a “one-handed” scientist lack rigor? How scientists discuss the work-relatedness of musculoskeletal disorders in formal and informal communications. Am J Ind Med 2008; 51: 173-85. doi: 10.1002/ajim.20547.
- Cofield S S, Corona R V, Allison D B. Use of causal language in observational studies of obesity and nutrition. Obes Facts 2010; 3: 353-6. doi: 10.1159/000322940.
- Shepard S, Checketts J, Eash C, Austin J, Arthur W, Wayant C, et al. Evaluation of spin in the abstracts of orthopedic trauma literature: a cross-sectional review. Injury 2021; 52: 1709-14. doi: 10.1016/j.injury.2021.04.060.
- Checketts J X, Riddle J, Zaaza Z, Boose M A, Whitener J H, Vassar M B. An evaluation of spin in lower extremity joint trials. J Arthroplasty 2019; 34: 1008-12. doi: 10.1016/j.arth.2019.01.016.
- Reddy A K, Lulkovich K, Wirtz A, Thompson J C, Scott J T, Checketts J X, et al. Assessment of spin in the abstracts of systematic reviews and meta-analyses on platelet-rich plasma treatment in orthopaedics: a cross-sectional analysis. Orthop J Sport.s Med 2023; 11. doi: 10.1177/23259671221137923
- Page M J, McKenzie J E, Bossuyt P M, Boutron I, Hoffmann T C, Mulrow C D, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ 2021; 372. doi: 10.1136/bmj.n71.