A comparison of cancellous screws in a sliding compression configuration and angle-stable sliding compression implants for internal fixation of femoral neck fractures in the non-elderly predominantly below 65 years: a systematic review and meta-analysis
Michaela M HANSEN 1,2, Mads S NIELSEN 1, Per H GUNDTOFT 3,4, Maiken STILLING 3,4, Ming DING 1,2, and Bjarke VIBERG 1,2
1 Department of Orthopaedic Surgery and Traumatology, Odense University Hospital; 2 Department of Clinical Medicine, University of Southern Denmark; 3 Department of Orthopaedic Surgery and Traumatology, Aarhus University Hospital; 4 Department of Clinical Medicine, Aarhus University, Denmark
Background and purpose — Internal fixation is the preferred treatment in the non-elderly with femoral neck fractures, regardless of fracture displacement. High complication rates are reported, in particular for displaced fractures. We aimed to compare cancellous screws with angle-stable sliding compression implants for internal fixation of femoral neck fractures in the non-elderly.
Methods — A systematic search was carried out in Medline, Embase, Scopus, and Cochrane. The search results were screened by 2 reviewers using Covidence and assessed for risk of bias. All comparative studies were included. The studies reported at least 1 of the following outcomes: avascular necrosis, fixation failure/cut-out, non-union, any complication, reoperation, femoral neck shortening, or Harris Hip Score (HHS). Dichotomous outcomes are reported as risk ratio (RR) and continuous outcomes as mean difference (MD). All effect measures use a random effects model.
Results — The search yielded 23 studies eligible for inclusion: 4 randomized controlled trials (RCTs) and 19 retrospective cohort trials, including 1,844 fractures. Only 1 study had low risk of bias. The results demonstrated no difference in RCTs alone. Analysis of all studies showed superior outcomes in favor of angle-stable sliding compression implants for fixation failure/cut-out (RR 0.54, 95% confidence interval [CI] 0.31–0.94), any complication (RR 0.49, CI 0.28–0.87), shortening > 5 mm (RR 0.54, CI 0.37–0.80), and HHS 6–24 months (MD 3.1, CI 1.8–4.4).
Conclusion — RCTs alone showed no significant differences between implant types. When including retrospective studies, angle-stable sliding compression implants demonstrated some advantages. The strength of evidence is limited by the predominance of retrospective cohort studies and high risk of bias in the included studies.
Citation: Acta Orthopaedica 2025; 96: 443–451. DOI: https://doi.org10.2340/17453674.2025.44034.
Copyright: © 2025 The Author(s). Published by MJS Publishing – Medical Journals Sweden, on behalf of the Nordic Orthopedic Federation. This is an Open Access article distributed under the terms of the Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0/).
Submitted: 2025-01-29. Accepted: 2025-05-26. Published: 2025-06-16.
Correspondence: michaela.manalili.hansen@rsyd.dk
MH: conceptualization, methodology, investigation, formal analysis, and writing—original draft. MN: investigation and writing—review & editing. MD, MS, PG: methodology and writing—review & editing. BV: conceptualization, methodology, writing—review & editing, and supervision.
Handling co-editors: Cecilia Rogmark and Robin Christensen
Acta thanks Simo Samuli Aukusti Miettinen and Jonas Sundkvist for help with peer review of this manuscript.
A femoral neck fracture is a detrimental health problem, affecting not only the elderly, but the young and middle-aged as well [1]. Several studies have demonstrated that non-elderly individuals with hip fractures often have impaired bone health. In a prospective study of patients aged 20–49 years, bone mass density was significantly lower compared with age-matched controls, regardless of trauma mechanism, suggesting underlying skeletal fragility [2]. Likewise, patients under 70 years of age have a high prevalence of osteoporosis, osteopenia, and significantly lower bone density [3,4].
Internal fixation is the preferred treatment for femoral neck fractures in the non-elderly due to its long-term performance and the risk of revision of hip arthroplasty [5,6]. However, a 5-year reoperation rate of 30% is reported after internal fixation [7]. When including only displaced femoral neck fractures the risk of failure can be as high as 59% [1]. Complications such as non-union, avascular necrosis, fixation failure, and femoral neck shortening are known adverse events [8-10].
There are a variety of implants for femoral neck fractures, but no clear consensus exists regarding which implant is superior in the management of femoral neck fractures in the non-elderly [11]. Several studies have evaluated implants for internal fixation of femoral neck fractures in the elderly [12]. Systematic reviews comparing cannulated cancellous screws (CCS) with sliding hip screw (SHS) or femoral neck system (FNS) show that SHS and FNS are associated with fewer postoperative complications across all age groups [13,14]. However, there are only a few studies comparing outcomes based on the type of implant used for internal fixation in the non-elderly [15].
Aiming for evidence-based clinical decision-making regarding internal fixation of femoral neck fractures in the non-elderly, typically below 65 years of age, in a systematic review and meta-analysis we compared clinical and functional outcomes of standard CCS with angle-stable sliding compression implants.
Methods
Design
This study was conducted as a systematic review and meta-analysis and was reported based on the Preferred Reporting Items for Systematic reviews and Meta-Analysis Protocols (PRISMA] guidelines [16].
Eligibility criteria
The inclusion criteria were based on the population/intervention/comparator/outcome/study design (PICOS) principle [17]:
- Population: Adults 18–69 years of age with femoral neck fracture.
- Intervention: Patients treated with CCS in a sliding compression configuration (triangle, inverted triangle, parallel).
- Comparator: Patients treated with any other angle-stable sliding compression implant.
- Outcomes: Studies that had at least 1 of the following outcomes: avascular necrosis, fixation failure/cut-out, non-union, any complication, reoperation, femoral neck shortening >5 mm, failure (not specified), pain Visual Rating Scale, Oxford Hip Score, Harris Hip Score (HHS), and 1-year mortality.
- Study design: RCTs, non-randomized controlled trials or quasi-randomized controlled trials, prospective cohort trials or retrospective comparative studies.
Exclusion criteria were:
- Full text not available in English, Danish, Norwegian, or Swedish.
- Less than 10 participants.
- Less than 6 months’ follow-up.
- Meeting abstracts, conference proceedings, biomechanical studies, animal studies, editorials, case reports/series, reviews, letters, surveys, expert opinions, non-comparative studies.
- Patient population with ipsilateral femur fractures.
- Studies reporting management using open reduction and/or grafting.
- Studies reporting delayed management and/or management of complications.
- Studies in which the relevant data could not be extracted (e.g., only P value reported or outcome not based on type of implant).
- Pediatric (<18 years) or elderly (≥70 years) population.
These studies would be excluded if the age of the study participants was not reported or if the age was reported only as a mean and the mean age +2 standard deviations was above 70 years of age. The cut-off at 70 years was chosen as the elderly are more likely to undergo arthroplasty rather than internal fixation, while non-elderly patients (<70 years) are more likely to benefit from preserving the native hip joint through internal fixation [6,18]. Furthermore, this age span was selected to reflect most existing studies, which typically report outcomes within this range and rarely use narrower age brackets.
In studies with mixed series, including for example both femoral neck fractures and intertrochanteric fractures or both non-elderly and elderly patients, only groups that met the inclusion criteria and had data for femoral neck fractures and/or patients <70 years of age reported separately were included in the study.
Information sources
A systematic literature search was carried out in April 2024 in Medline, Embase, Scopus, and Cochrane. The reference lists of the studies extrapolated from full text screening were manually screened for additional eligible studies.
Search strategy
A comprehensive search string was built under guidance of a research librarian and adjusted to each specific database, to identify studies on internal fixation of femoral neck fractures. MeSH terms and keywords related to femoral neck fractures and internal fixation were used. The search string was validated by identifying 3 preselected relevant articles and confirming that they were identified using the search string [19-21]. No terms regarding age were used, and studies with a patient population ≥70 years of age were excluded manually during screening. A full description of the search strategy for each database may be found in Supplementary data.
Selection process
Screening was conducted using Covidence systematic review software (Veritas Health Innovation, Melbourne, Australia). The Covidence software was used to automatically remove duplicates before screening. The titles and abstracts were screened independently by reviewers MH and MN after the automatic removal of duplicates. If a title clearly did not meet the eligibility criteria, the study was excluded on title alone. If the title in any way indicated eligibility, the abstract was screened. The reviewers erred on the side of inclusivity and if the abstract did not contain enough information to exclude the study, the full text was screened. Full text screening was conducted independently by the same 2 reviewers, MH and MN, and excluded studies were classified according to the reason for exclusion. In the case of discrepancy the eligibility was discussed between the 2 reviewers and, if necessary, with the other co-authors.
Data collection process and data items
Data was collected by 2 reviewers using a prefabricated data extraction form. The following study characteristics were extracted from the eligible studies: title, authors, publication year, journal, country, study design, target population, mean age, sample size of each group, implants used for internal fixation, and follow-up duration. The clinical outcomes extracted were: avascular necrosis, fixation failure/cut-out, non-union, any complication, reoperation, femoral neck shortening >5 mm [22], failure (not specified), pain Visual Rating Scale, Oxford Hip Score, HHS, and 1-year mortality. The functional outcomes were extracted for 6–24 months and >24 months.
Synthesis methods
RCTs are reported both separately and pooled with retrospective cohort studies. The studies were eligible for synthesis if at least 1 of the prespecified outcomes was reported. The functional outcomes had to be reported for follow-up at either 6–24 months or >24 months. Femoral neck shortening had to be defined as >5 mm. If the shortening was not defined, it would not be included in analysis.
Study risk of bias assessment
Risk of bias assessment was performed by 2 reviewers using Cochrane’s tools for risk of bias assessment RoB2 [23] and ROBINS-I [24]. For each domain, 3 measurements were used. Any disagreement in risk of bias assessment was resolved between the 2 reviewers.
Reporting bias assessment
Clinical trial registers and protocols were screened to assess outcome reporting bias for the included studies. Funnel plots were used to assess publication bias for outcomes with more than 10 studies.
Statistics
Statistical analysis was performed using RevMan v8.19.0 (https://training.cochrane.org/online-learning/core-software) [25]. Dichotomous outcomes were analyzed using inverse variance with risk ratio as the effect measure. Continuous outcomes were analyzed using inverse variance with mean difference as the effect measure. The analyses use random effect models, as the data are assumed to have heterogeneity. Heterogeneity was estimated using Restricted Maximum-Likelihood [26]. All outcomes are reported with a 95% confidence interval (CI) using a Wald-type method.
Ethics, registration, data sharing plan, funding, and disclosures
No ethical approval was needed. The protocol was registered in PROSPERO, the international prospective register of systematic reviews (CRD42024498684). The protocol has been amended to specify the intervention/comparator as CCS compared with angle-stable sliding compression implants and not “any” implant, as the search yielded several reports on non-sliding length stable implants. There were enough reports for a secondary review focusing on internal fixation with sliding compression cannulated cancellous screws compared with non-sliding implants. The strategy for data synthesis has been updated to be more specific and described in detail prior to data synthesis.
Femoral neck shortening has been added as an outcome because it is an implied postoperative complication closely related to fixation failure and functional outcomes. While it was not explicitly registered in PROSPERO, femoral neck shortening is an intermediary outcome that may contribute to fixation failure, non-union, and poor functional scores. We believe its inclusion strengthens the analysis rather than diverging from the registered outcomes. This addition does not alter the study’s primary objectives but provides further insight.
Data is available upon reasonable request through the corresponding author.
This systematic review is part of a PhD project supported by the Region of Southern Denmark’s fund to support clinical doctoral candidates. The funder has no role in the design, analysis, data interpretation, or decision to submit results.
No competing interests are reported. Complete disclosure of interest forms according to ICMJE are available on the article page, doi: 10.2340/17453674.2025.44034
Results
Study selection
9,973 reports were screened for title/abstract and 126 were full text screened. The screening yielded 23 studies [19-21,27-46] eligible for inclusion (Figure 1) [47].
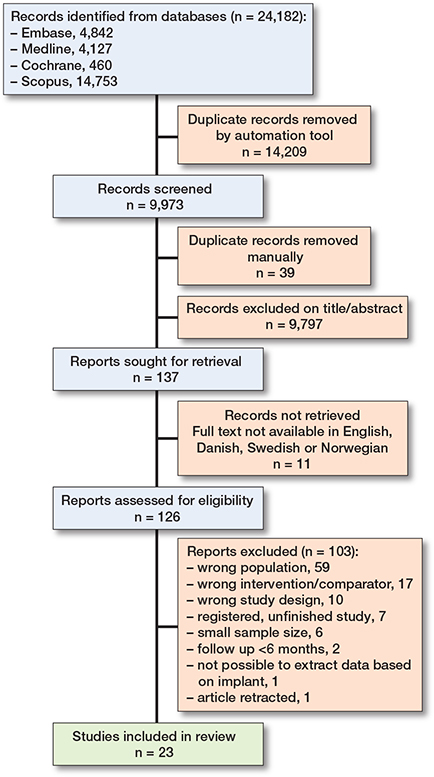
Most full text screened records were excluded due to the population being ≥70 years of age or not being femoral neck fractures. Other reasons for exclusion were the study not being comparative or that the intervention or comparator did not align with the inclusion and exclusion criteria. Most studies were excluded for more than 1 reason. We identified 1 ongoing study not yet recruiting [48].
Study characteristics
Our review includes 1,844 patients from 23 studies of which 4 are RCTs and 19 are retrospective cohort studies (Table 1). The control group consists of CCS in a sliding compression configuration. The experimental group consists of Targon Locking plate, SHS ± derotation screw, and FNS ± derotation screw.
| Reference | Design | Country | Sample size | Age | Fracture classification | Follow-up (months) | Experimental |
| Hegazy 2023 [32] | RCT | Egypt | 50 | 18–60 | Garden I–IV | 12–36 | TFN |
| Siavashi 2015 [39] | RCT | Iran | 58 | 18–60 | Garden III–IV | 12–36 | SHS + derotation screw |
| FAITH trial 2017 [46] | RCT | International | 221 | 50–60 | ND | 24 | SHS |
| Gupta 2016 [30] | PCS | India | 85 | 16–60 | Garden I–IV | 48 | SHS |
| He 2021 [31] | RCS | China | 69 | 18–65 | Garden I–IV | 17 | FNS |
| Hu 2021 [19] | RCS | China | 44 | <60 | All | 12 | FNS |
| Huang 2023 [33] | RCS | China | 87 | <65 | Garden III–IV | 12 | FNS |
| Pauwel III | |||||||
| Kenmegne 2023 [20] | RCS | China | 114 | 18–65 | All | 12–36 | FNS |
| Yan 2023 [21] | RCS | China | 49 | 18–60 | All | 21–24 | FNS |
| Zhang 2022 [44] | RCS | China | 69 | <65 | Garden II–IV | 6 | FNS |
| Zhou 2021 [45] | RCS | China | 60 | <65 | Pauwel III | 10–22 | FNS |
| Su 2023 [41] | RCS | China | 129 | 18–65 | All | 12 | FNS ± derotation screw |
| Cai 2024 [28] | RCS | China | 120 | <65 | All | 12 | SHS and FNS |
| Xu 2023 [43] | RCS | China | 65 | 18–60 | All | 12 | SHS and FNS |
| Gardner 2015 [29] | RCS | USA | 69 | <60 | Garden III–IV | 11–30 | SHS |
| Kaplan 2012 [35] | RCS | Turkey | 66 | 18–68 | Garden I–IV | 7–57 | SHS |
| Lim 2024 [36] | RCS | Singapore | 57 | 16–64 | All | 12 | SHS |
| Liporace 2008 [37] | RCS | USA | 46 | 19–64 | Pauwel III | 19–36 | SHS |
| Jiang 2021 [34] | RCS | China | 139 | 20–60 | Garden I–IV | >24 | SHS + derotation screw |
| Pauwel II–III | |||||||
| Stockton 2019 [40] | RCS | USA | 201 | 18–55 | Garden III–IV | N/A | SHS + derotation screw |
| Bouaicha 2023 [27] | RCS | Tunisia | 72 | 18–65 | Garden I–IV | >24 | SHS ± derotation screw |
| Razik 2012 [38] | RCS | UK | 92 | <60 | Garden I–IV | 24 | SHS ± derotation screw |
| Warschawski 2021 [42] | RCS | Israel | 103 | <65 | Garden III–IV | 84 | TFN |
| RCT: randomized controlled trial, PCS: prospective comparative study, RCS: retrospective cohort study, ND: no data, SHS: sliding hip screw, FNS: femoral neck system, TFN: Targon femoral neck locking plate | |||||||
Risk of bias in studies
The included studies are considered to have moderate to high risk of bias (Tables 2 and 3). Only 1 RCT is rated as low risk, while 2 others raise concerns regarding the randomization due to unclear methodology [30,39]. Domain 2 is inadequately reported in these 2 studies, and 1 study documents crossover without detailing deviations among participants aged 50–60 years [46]. None of the studies report missing outcome data. Bias in the measurement of outcome is considered low risk when the outcomes are clearly defined, minimizing the risk of bias.
Table 2. Risk of bias assessment of randomized studies, RoB 2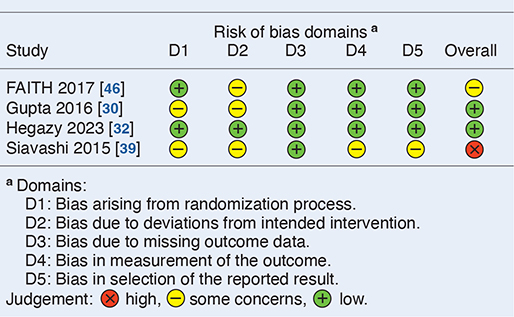
Table 3. Risk of bias assessment of retrospective cohort studies, ROBINS-I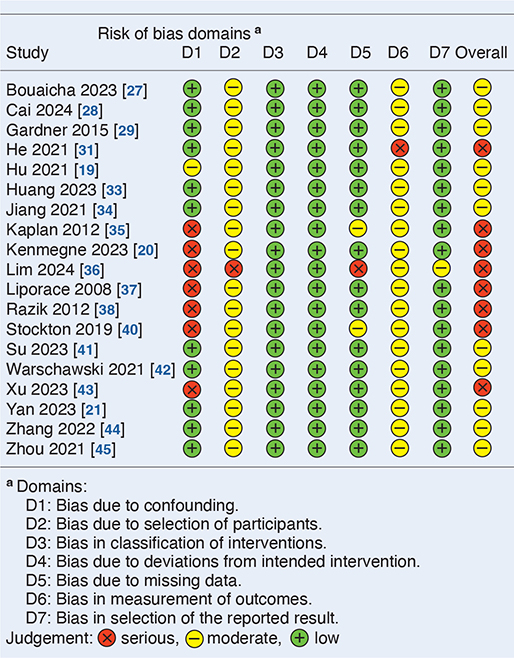
In the retrospective cohort studies, the main risks of bias are confounding, selection bias, and outcome measurement bias. Confounding arises from differences in patient characteristics such as fracture displacement, age, reduction quality, and comorbidities. Selection bias stems from non-randomized treatments, and the retrospective design inherently excluding patients with incomplete follow-up. Intervention classification is clearly defined and adherence to treatment is not considered relevant. Outcome measures are influenced by the assessor’s awareness of the intervention, resulting in moderate concerns for outcome measurement bias.
Results of individual studies
Avascular necrosis, fixation failure, non-union, and reoperation were the only outcomes reported by RCTs. The most reported outcomes were avascular necrosis, fixation failure/cut out, and non-union, which were reported by 18, 17, and 15 studies, respectively.
None of the included studies report Oxford Hip Score, pain Visual Rating Scale, or 1-year mortality.
Results of syntheses
The detailed results are shown in Table 4 and Figures 2–5. Results from combined analyses may be found in the Supplementary data. Meta-analysis on RCTs alone demonstrates no significant differences. The meta-analysis that included retrospective cohort studies shows a significant difference in risk ratio of fixation failure/cut out, any complication, and shortening >5 mm in favor of angle-stable sliding compression implants as well as a significant difference in weighted mean difference in HHS at 6–24 months in favor of angle-stable sliding compression implants. All studies reporting HHS at 6–24 months are comparisons between CCS and FNS. Cai et al. report comparisons of HHS between CCS, FNS, and SHS [28].
| Outcomes | Sample size | Risk ratio (CI) | I2 % | P value | ||
| Studies n | Angle stable | CCS | ||||
| Randomized trials | ||||||
| Avascular necrosis | 3 | 95 | 98 | 0.88 (0.31–2.5) | 0 | 0.8 |
| Fixation failure/cut-out | 2 | 70 | 73 | 0.47 (0.03–6.9) | 68 | 0.6 |
| Non-union | 2 | 65 | 70 | 0.59 (0.25–1.4) | 0 | 0.2 |
| Reoperation | 2 | 132 | 147 | 0.71 (0.41–1.2) | 0 | 0.2 |
| All studies | ||||||
| Avascular necrosis | 18 | 711 | 752 | 1.0 (0.70–1.4) | 12 | 1 |
| Fixation failure/cut-out | 17 | 736 | 794 | 0.54 (0.31–0.94) | 33 | 0.03 |
| Non-union | 15 | 516 | 594 | 0.64 (0.39–1.1) | 21 | 0.08 |
| Any complication | 7 | 233 | 230 | 0.49 (0.28–0.87) | 47 | 0.02 |
| Reoperation | 6 | 336 | 292 | 0.85 (0.58–1.3) | 0 | 0.4 |
| Shortening > 5 mm | 5 | 260 | 240 | 0.54 (0.37–0.80) | 32 | 0.002 |
| Failure, unspecified | 3 | 156 | 253 | 0.83 (0.57–1.1) | 0 | 0.3 |
| Harris Hip Score a | ||||||
| 6–24 months | 8 | 317 | 310 | 3.1 (1.8 to 4.4) a | 70 | <0.001 |
| > 24 months | 2 | 93 | 149 | 1.7 (–3.1 to 6.4) a | 0 | 0.5 |
| aMean difference. | ||||||
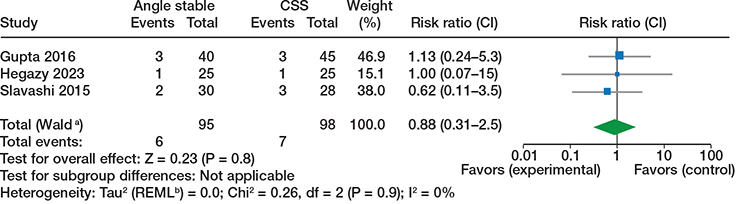
Figure 2. Avascular necrosis, randomized trials. Analyses used inverse variance with risk ratio as outcome with random effect models. CSS = cannulated cancellous screws, CI = 95% confidence interval. a CI calculated by Wald-type method. b Tau2 calculated by Restricted Maximum-Likelihood method.
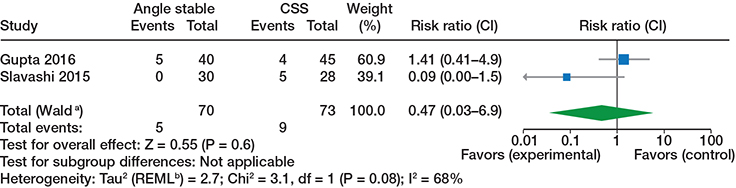
Figure 3. Fixation failure/cut out, randomized trials, see comments in Figure 2.
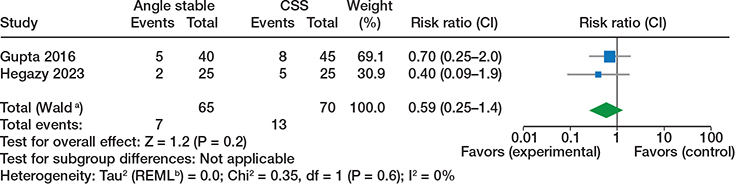
Figure 4. Non-union, randomized trials, see comments in Figure 2.

Figure 5. Reoperation, see comments in Figure 2.
Reporting biases
Funnel plots of outcomes reported in 10 or more studies do not indicate reporting bias (see Supplementary data).
Discussion
General interpretation of results in context of other evidence
This systematic review and meta-analysis included 23 studies with 1,844 patients, the majority being below 65 years of age. The analysis of RCTs alone demonstrated no significant differences between CCS and angle-stable sliding compression implants for any outcome. When including retrospective cohort studies, angle-stable sliding compression implants were associated with an approximately 50% reduction in the risk of fixation failure/cut-out, overall complications, and femoral neck shortening > 5mm.
Albeit based on lower evidence, we find reduction in fixation failure/cut-out relevant as it supports the biomechanical advantage of angle-stable sliding compression implants, offering a degree of clinical confirmation for biomechanical expectations, even if causality cannot be firmly established. The increased stability and controlled dynamic compression provided by these implants likely contribute to reducing the risk of fixation failure, particularly in fractures prone to shearing forces [49,50].
Similarly, the reduction in overall complications and femoral neck shortening > 5mm aligns with existing literature, which associates shortening with inferior functional outcomes, gait abnormalities, and increased risk of osteoarthritis [10,51].
Although RCTs showed no differences in HHS, the combined analysis suggests a small improvement in HHS at 6–24 months postoperatively in favor of angle-stable sliding compression implants but not a clinically important difference [52].
It is also important to consider the heterogeneous population included in this review. While adults younger than 70 years of age may possess higher baseline physiological reserves, several studies indicate that this group does not necessarily experience better outcomes. A qualitative study highlighted persistent disability and pain years after surgery in patients under 60, in part due to rehabilitation programs geared toward older populations [53]. Furthermore, non-elderly adults who suffer hip fractures often have comorbidities and lifestyle risk factors such as smoking and alcohol use, which adversely impact both bone health and rehabilitation potential [1]. In this context, chronological age is a poor surrogate for biological age, as many patients resemble the elderly in terms of bone quality, general health, and rehabilitation potential, with only a minority being truly fit and active. Therefore, the wide age span in the included studies is less important than the underlying biological variability, which must be acknowledged to enable meaningful subgroup analyses.
Limitations of evidence
The evidence in this review is limited by the predominance of non-randomized retrospective cohort studies, increasing risks of confounding, selection bias, and inaccurate outcome measurement [54]. Only 1 RCT is rated as low risk of bias, weakening the strength of conclusions. Although RCTs are preferred, their scarcity requires the inclusion of cohort studies for greater sample diversity and to assess complications and functional outcomes, despite inherent biases [55,56].
The use of both prospective and retrospective studies adds heterogeneity due to varying methodologies and follow-up, but this provides broader insights where RCT data ise insufficient [56].
Additionally, a key limitation is the inability to perform a subgroup analysis based on fracture displacement. While it would be ideal to separate undisplaced (Garden I–II) and displaced (Garden III–IV) fractures, the classification methods in the included studies are inconsistent. Of the 23 studies, only 5 specifically report on Garden III–IV fractures, while 14 include all fracture types. 1 study does not provide a classification, 1 includes Garden II–IV, and 2 report only on Pauwels III fractures without referencing the Garden classification. This variation in reporting prevents a reliable comparison based on displacement.
Another important limitation is the substantial biological variability within the included patient population. Although the age range (18–69 years) appears wide, the real issue lies in the heterogeneity in bone quality, comorbidities, and functional capacity across individuals, which is not adequately captured by chronological age alone. Ideally, analyses would stratify patients based on relevant biological or clinical profiles, but this was not feasible with the available studies. Therefore, the age span—and the biological variability it contains—reflects the current state of the literature rather than a methodological choice.
The methods used for measuring femoral neck shortening in the included studies lack sufficient accuracy. Incorporating radiostereometric analysis into clinical trials could allow for more reliable assessment of femoral neck shortening as well as provide high precision and detailed insights into both implant and fracture migration [57].
Limitations of review process
Despite a systematic approach, several factors may limit comprehensiveness. Of 9,973 screened reports, only 23 meet the inclusion criteria. Manual selection by 2 reviewers, although thorough, introduce subjective judgment risks, and strict age limits (<70 years) exclude potentially relevant studies. Excluding studies with languages outside English, Danish, Norwegian, and Swedish may have introduced language bias. Funnel plot analyses are constrained to outcomes from 10 or more studies, possibly overlooking publication bias in areas with fewer studies.
Conclusion
High-level evidence alone showed no significant differences between implant types for internal fixation of femoral neck fractures in the non-elderly. When incorporating lower quality evidence, angle-stable sliding compression implants may demonstrate some advantages in reducing fixation failure and overall complications compared with CCS. However, the strength of evidence is limited by the predominance of retrospective cohort studies, high heterogeneity of studies, and high risk of bias.
Supplementary data
Search strings and Figures A–L are available as Supplementary data on the article homepage, doi: 10.2340/17453674.2025.44034
- Rogmark C, Kristensen M T, Viberg B, Rönnquist S S, Overgaard S, Palm H. Hip fractures in the non-elderly: who, why and whither? Injury 2018; 49(8): 1445-50. doi: 10.1016/j.injury.2018.06.028.
- Lofthus C M, Osnes E K, Meyer H E, Kristiansen I S, Nordsletten L, Falch J A. Young patients with hip fracture: a population-based study of bone mass and risk factors for osteoporosis. Osteoporos Int 2006; 17(11): 1666-72. doi: 10.1007/s00198-006-0176-0.
- Strøm Rönnquist S, Viberg B, Kristensen M T, Palm H, Jensen J B, Madsen C F, et al. Frailty and osteoporosis in patients with hip fractures under the age of 60: a prospective cohort of 218 individuals. Osteoporos Int 2022; 33(5): 1037-55. doi: 10.1007/s00198-021-06281-y.
- Bartels S, Gjertsen J E, Frihagen F, Rogmark C, Utvåg S E. Low bone density and high morbidity in patients between 55 and 70 years with displaced femoral neck fractures: a case-control study of 50 patients vs 150 normal controls. BMC Musculoskelet Disord 2019; 20(1): 371. doi: 10.1186/s12891-019-2732-8.
- Bhandari M, Swiontkowski M. Management of acute hip fracture. N Engl J Med 2017; 377(21): 2053-62. doi: 10.1016/j.mporth.2016.10.004.
- Goudie E B, Duckworth A D, White T O. Hip fractures in young adults. Orthop Trauma 2017; 31(2): 76-85. doi: 10.1016/j.mporth.2016.10.004.
- Stockton D J, O’Hara L M, O’Hara N N, Lefaivre K A, O’Brien P J, Slobogean G P. High rate of reoperation and conversion to total hip arthroplasty after internal fixation of young femoral neck fractures: a population-based study of 796 patients. Acta Orthop 2019; 90(1): 21-5. doi: 10.1080/17453674.2018.1558380.
- Hayat Z, Varacallo M. Surgical Management of Femoral Neck Fractures. StatPearls. Treasure Island, FL: StatPearls Publishing. Copyright © 2024, StatPearls Publishing LLC; 2024. PMID: 30855824.
- Slobogean G P, Sprague S A, Scott T, Bhandari M. Complications following young femoral neck fractures. Injury 2015; 46(3): 484-91. doi: 10.1016/j.injury.2014.10.010.
- Slobogean G P, Stockton D J, Zeng B F, Wang D, Ma B, Pollak A N. Femoral neck shortening in adult patients under the age of 55 years is associated with worse functional outcomes: analysis of the prospective multi-center study of hip fracture outcomes in China (SHOC). Injury 2017; 48(8): 1837-42. doi: 10.1016/j.injury.2017.06.013.
- Slobogean G P, Sprague S A, Scott T, McKee M, Bhandari M. Management of young femoral neck fractures: is there a consensus? Injury 2015; 46(3): 435-40. doi: 10.1016/j.injury.2014.11.028.
- Lewis S R, Macey R, Eardley W G, Dixon J. R, Cook J, Griffin X L. Internal fixation implants for intracapsular hip fractures in older adults. Cochrane Database Syst Rev 2021; 3(3): Cd013409. doi: 10.1002/14651858.CD013409.pub2.
- Ma J X, Kuang M J, Xing F, Zhao Y L, Chen H T, Zhang L K, et al. Sliding hip screw versus cannulated cancellous screws for fixation of femoral neck fracture in adults: a systematic review. Int J Surg 2018; 52: 89-97. doi: 10.1016/j.ijsu.2018.01.050.
- Zhou Y, Li Z, Lao K, Wang Z, Zhang L, Dai S, et al. Femoral neck system vs. cannulated screws on treating femoral neck fracture: a meta-analysis and system review. Front Surg 2023; 10. doi: 10.3389/fsurg.2023.1224559.
- Peng P, Xiao F, He X, Fang W, Huang J, Wang B, et al. Global research status and trends of femoral neck fracture over the past 27 years: a historical review and bibliometric analysis. Front Surg 2022; 9:875040. doi: 10.3389/fsurg.2022.875040.
- Moher D, Liberati A, Tetzlaff J, Altman D G. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med 2009; 6(7): e1000097. doi: 10.1371/journal.pmed.1000097.
- O’Connor D, Green S, Higgins P T. Defining the review question and developing criteria for including studies. In: Higgins PT, Green S, editors. Cochrane Handbook for Systematic Reviews of Interventions: Cochrane Book Series. Chichester: Wiley; 2008. p. 81-94. doi: 10.1002/9780470712184.ch5.
- Ly T V, Swiontkowski M F. Management of femoral neck fractures in young adults. Indian J Orthop 2008; 42(1): 3-12. doi: 10.4103/0019-5413.38574.
- Hu H, Cheng J, Feng M, Gao Z, Wu J, Lu S. Clinical outcome of femoral neck system versus cannulated compression screws for fixation of femoral neck fracture in younger patients. J Orthop Surg Res 2021; 16(1): 370. doi: 10.1186/s13018-021-02517-z.
- Kenmegne G R, Zou C, Fang Y, He X, Lin Y, Yin Y. Femoral neck fractures in non-geriatric patients: femoral neck system versus cannulated cancellous screw. BMC Musculoskelet Disord 2023; 24(1): 70. doi: 10.1186/s12891-023-06140-3.
- Yan S G, Cui Y, Li D, Liu F, Hua X, Schmidutz F. Femoral neck system versus three cannulated screws for fixation of femoral neck fractures in younger patients: a retrospective cohort study. J Invest Surg 2023; 36(1): 2266752. doi: 10.1080/08941939.2023.2266752.
- Felton J, Slobogean G P, Jackson S S, Della Rocca G J, Liew S, Haverlag R, et al. Femoral neck shortening after hip fracture fixation is associated with inferior hip function: results from the FAITH trial. J Orthop Trauma 2019; 33(10): 487-96. doi: 10.1097/BOT.0000000000001551.
- Sterne J A C, Savović J, Page M J, Elbers R G, Blencowe N S, Boutron I, et al. RoB 2: a revised tool for assessing risk of bias in randomised trials. BMJ 2019; 366: l4898. doi: 10.1136/bmj.l4898.
- Sterne J A, Hernán M A, Reeves B C, Savović J, Berkman N D, Viswanathan M, et al. ROBINS-I: a tool for assessing risk of bias in non-randomised studies of interventions. BMJ 2016; 355: i4919. doi: 10.1136/bmj.i4919.
- Review Manager (RevMan). 8.19.0 ed. The Cochrane Collaboration; 2025. Available from: http://www.revman.cochrane.org
- Langan D, Higgins J P T, Jackson D, Bowden J, Veroniki A A, Kontopantelis E, et al. A comparison of heterogeneity variance estimators in simulated random-effects meta-analyses. Res Synth Methods 2019; 10(1): 83-98. doi: 10.1002/jrsm.1316.
- Bouaicha W, Jlidi M, Elarbi M, Mallek K, Jaziri S, Abdennadher A, et al. Surgical management of neck of femur fractures in patients younger than sixty-five years: a comparative study of three fixation methods. Int Orthop 2023; 47(12): 3099-106. doi: 10.1007/s00264-023-05997-2.
- Cai L, Zheng W, Chen C, Hu W, Chen H, Wang T. Comparison of young femoral neck fractures treated by femoral neck system, multiple cancellous screws and dynamic hip screws: a retrospectively comparison study. BMC Musculoskelel Disord 2024; 25(1): 188. doi: 10.1186/s12891-024-07319-y.
- Gardner S, Weaver M J, Jerabek S, Rodriguez E, Vrahas M, Harris M. Predictors of early failure in young patients with displaced femoral neck fractures. J Orthop 2015; 12(2): 75-80. doi: 10.1186/s12891-024-07319-y.
- Gupta M, Arya R K, Kumar S, Jain V K, Sinha S, Naik A K. Comparative study of multiple cancellous screws versus sliding hip screws in femoral neck fractures of young adults. Chin J Traumatol 2016; 19(4): 209-12. doi: 10.1016/j.cjtee.2015.11.021.
- He C, Lu Y, Wang Q, Ren C, Li M, Yang M, et al. Comparison of the clinical efficacy of a femoral neck system versus cannulated screws in the treatment of femoral neck fracture in young adults. BMC Musculoskelet Disord 2021; 22(1): 994. doi: 10.1186/s12891-021-04888-0.
- Hegazy A A F, Morsy A M, Elbana E, Abdelkader M A. Management of intracapsular neck femur fracture by Targon plate versus cannulated screws. J Pharmac Negat Results 2023; 14(2): 650-6. doi: 10.47750/pnr.2023.14.02.81.
- Huang S, Zhang Y, Zhang X, Zhou C, Li W, Wang Y, et al. Comparison of femoral neck system and three cannulated cancellous screws in the treatment of vertical femoral neck fractures: clinical observation and finite element analysis. BioMed Eng Online 2023; 22(1): 20. doi: 10.1186/s12938-023-01083-1.
- Jiang D, Zhan S, Cai Q, Hu H, Jia W. Enhanced interfragmentary stability and improved clinical prognosis with use of the off-axis screw technique to treat vertical femoral neck fractures in nongeriatric patients. J Orthop Surg Res 2021; 16(1): 473. doi: 10.1186/s13018-021-02619-8.
- Kaplan T, Akesen B, Demirag B, Bilgen S, Durak K. Comparative results of percutaneous cannulated screws, dynamic compression type plate and screw for the treatment of femoral neck fractures. Ulusal Travma Acil Cerrahi Derg 2012; 18(1): 65-70. doi: 10.5505/tjtes.2011.33427.
- Lim Z Z C, Tan C M P, Antony Xavier R P, Yam M G J, Chua I T H. Femoral neck system as a safe alternative to cannulated compression screw and dynamic hip screw in femoral neck fractures: an early comparative study. Singapore Med J 2024. doi: 10.4103/singaporemedj.SMJ-2022-024.
- Liporace F, Gaines R, Collinge C, Haidukewych G J. Results of internal fixation of Pauwels type-3 vertical femoral neck fractures. J Bone Joint Surg Am 2008; 90(8): 1654-9. doi: 10.2106/JBJS.G.01353.
- Razik F, Alexopoulos A S, El-Osta B, Connolly M J, Brown A, Hassan S, et al. Time to internal fixation of femoral neck fractures in patients under sixty years: does this matter in the development of osteonecrosis of femoral head? Int Orthop 2012; 36(10): 2127-32. doi: 10.1007/s00264-012-1619-1.
- Siavashi B, Aalirezaei A, Moosavi M, Golbakhsh M R, Savadkoohi D, Zehtab M J. A comparative study between multiple cannulated screws and dynamic hip screw for fixation of femoral neck fracture in adults. Int Orthop 2015; 39(10): 2069-71. doi: 10.1007/s00264-015-2881-9.
- Stockton D J, Dua K, O’Brien P J, Pollak A N, Hoshino C M, Slobogean G P. Failure patterns of femoral neck fracture fixation in young patients. Orthopedics 2019; 42(4): E376-E80. doi: 10.3928/01477447-20190321-03.
- Su M, He Z, Huang N, Lin X, Fang K, Dai Z. Superior short-term outcomes of FNS in combination with a cannulated screw in treating femoral neck fractures. BMC Musculoskelet Disord 2023; 24(1): 823. doi: 10.1186/s12891-023-06959-w.
- Warschawski Y, Rutenberg T F, Factor S, Tudor A, Sharfman Z, Morgan S, et al. Dynamic locking plate vs. cannulated cancellous screw for displaced intracapsular hip fracture: a comparative study. J Orthop 2021; 24: 15-18. doi: 10.1016/j.jor.2021.02.008.
- Xu X, Fan J, Zhou F, Lv Y, Tian Y, Ji H, et al. Comparison of femoral neck system to multiple cancellous screws and dynamic hip screws in the treatment of femoral neck fractures. Injury 2023; 54(Suppl 2) (0226040, gon): S28-S35. doi: 10.1016/j.injury.2022.03.041.
- Zhang Y Z, Lin Y, Li C, Yue X J, Li G Y, Wang B, et al. A comparative analysis of femoral neck system and three cannulated screws fixation in the treatment of femoral neck fractures: a six-month follow-up. Orthop Surg 2022; 14(4): 686-93. doi: 10.1111/os.13235.
- Zhou X Q, Li Z Q, Xu R J, She Y S, Zhang X X, Chen G X, et al. Comparison of early clinical results for femoral neck system and cannulated screws in the treatment of unstable femoral neck fractures. Orthop Surg 2021; 13(6): 1802-9. doi: 10.1111/os.13098.
- FAITH investigators. Fracture fixation in the operative management of hip fractures (FAITH): an international, multicentre, randomised controlled trial. Lancet 2017; 389(10078): 1519-27. doi: 10.1016/S0140-6736(17)30066-1.
- Haddaway N R, Page M J, Pritchard C C, McGuinness L A. PRISMA2020: An R package and Shiny app for producing PRISMA 2020-compliant flow diagrams, with interactivity for optimised digital transparency and Open Synthesis. Campbell Syst Rev 2022; 18(2): e1230. doi: 10.1002/cl2.1230.
- Ahmed I M. Femoral neck locking plate vs multiple cannulated cancellous screws in treatment of femoral neck fractures in young adults: randomized controlled clinical trial study 2023 [updated 2023-12-19]. Available from: https://clinicaltrials.gov/study/NCT06162637
- Brattgjerd J E, Steen H, Strømsøe K. Increased stability by a novel femoral neck interlocking plate compared to conventional fixation methods: a biomechanical study in synthetic bone. Clin Biomech (Bristol, Avon) 2020; 76:104995. doi: 10.1016/j.clinbiomech.2020.104995.
- Schopper C, Zderic I, Menze J, Müller D, Rocci M, Knobe M, et al. Higher stability and more predictive fixation with the Femoral Neck System versus Hansson Pins in femoral neck fractures Pauwels II. J Orthop Translat 2020; 24: 88-95. doi: 10.1016/j.jot.2020.06.002.
- Lee D H, Kwon J H, Kim K C. The effects and risk factors of femoral neck shortening after internal fixation of femoral neck fractures. Clin Orthop Surg 2024; 16(5): 718-23. doi: 10.4055/cios24089.
- Achten J, Parsons N, Edlin R, Griffin D, Costa M. A randomised controlled trial of total hip arthroplasty versus resurfacing arthroplasty in the treatment of young patients with arthritis of the hip joint. BMC Musculoskelet Disord 2010; 11: 8. doi: 10.1186/1471-2474-11-8.
- Strøm Rönnquist S, Svensson H K, Jensen C M, Overgaard S, Rogmark C. Lingering challenges in everyday life for adults under age 60 with hip fractures: a qualitative study of the lived experience during the first three years. Int J Qual Stud Health Well-being 2023; 18(1): 2191426. doi: 10.1080/17482631.2023.2191426.
- Higgins J P, Ramsay C, Reeves B C, Deeks J J, Shea B, Valentine J C, et al. Issues relating to study design and risk of bias when including non-randomized studies in systematic reviews on the effects of interventions. Res Synth Methods 2013; 4(1): 12-25. doi: 10.1002/jrsm.1056.
- Schünemann H J, Tugwell P, Reeves B C, Akl E A, Santesso N, Spencer F A, et al. Non-randomized studies as a source of complementary, sequential or replacement evidence for randomized controlled trials in systematic reviews on the effects of interventions. Res Synth Methods 2013; 4(1): 49-62. doi: 10.1002/jrsm.1078.
- Audigé L, Bhandari M, Griffin D, Middleton P, Reeves B C. Systematic reviews of nonrandomized clinical studies in the orthopaedic literature. Clin Orthop Relat Res 2004(427): 249-57. doi: 10.1097/01.blo.0000137558.97346.fb.
- Kaptein B L, Pijls B, Koster L, Kärrholm J, Hull M, Niesen A, et al. Guideline for RSA and CT-RSA implant migration measurements: an update of standardizations and recommendations. Acta Orthop 2024; 95: 256-67. doi: 10.2340/17453674.2024.40709.