Association of resident training with complication risk in total hip and knee arthroplasty: a systematic review and meta-analysis
Diederik H R KEMPEN 1,2, Barry VAN DER ENDE 1, Diyar DELAWI 3, Chantal DEN HAAN 4, Amy HOFMAN 4, Rudolf W POOLMAN 1,5, and Nienke WOLTERBEEK 3
1 Department of Orthopedic Surgery, Joint Research, OLVG Amsterdam, Amsterdam; 2 Department of Orthopedic Surgery, Amsterdam University Medical Center, Amsterdam; 3 Department of Orthopedic Surgery, St. Antonius Hospital, Utrecht; 4 Department of Research and Epidemiology, OLVG Amsterdam, Amsterdam; 5 Department of Orthopaedic Surgery, Leiden University Medical Center, Leiden, The Netherlands
Background and purpose — An important aspect of orthopedic residency is to gain experience and perform total joint arthroplasties to learn operating skills. For patients, a substantial concern is that resident involvement may result in more adverse events. We performed a systematic review with meta-analysis to evaluate whether resident involvement is associated with a higher complication rate in total hip and knee arthroplasty compared with procedures performed by orthopedic surgeons.
Methods — PubMed, Embase, Central, Cinahl, and Web of Science were systematically searched until November 2, 2023. Studies were assessed by 2 reviewers independently. All manuscripts were included describing: (i) complications in total hip and/or knee arthroplasty and (ii) comparing procedures with and without resident involvement.
Results — 29 studies could be included with a MINORS score ranging from 10 to 17. Resident involvement could not be associated with an increased overall and surgical complication rate in 9 (n = 51,442 patients) and 12 studies (n = 37,789 patients), respectively. The meta-analysis for deep infection showed an association with resident involvement (RR 1.55, 95% confidence interval 1.09–2.20, P = 0.01, 18 studies). In single studies, associations were seen for any urologic complication and sepsis. All other complications could not be related to resident involvement.
Conclusion — This systematic review could not find evidence that resident involvement was associated with more overall complications or surgical site complications except for deep infection. As previous studies showed an increased infection risk with prolonged duration of the procedure, consultants in teaching hospitals should be aware of this risk and be alert to teaching time to limit the risk for patients.
Citation: Acta Orthopaedica 2025; 96: 850–856. DOI: https://doi.org/10.2340/17453674.2025.43905.
Copyright: © 2025 The Author(s). Published by MJS Publishing – Medical Journals Sweden, on behalf of the Nordic Orthopedic Federation. This is an Open Access article distributed under the terms of the Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0/)
Submitted: 2023-12-31. Accepted: 2025-05-16. Published: 2025-11-17.
Correspondence: d.h.r.kempen@olvg.nl
All co-authors (DK, BE, DD, CdH, AH, RP, NW) contributed to the concept and design of the study. CdH performed the literature search, DK and NW performed the study selection and data extraction. DK, BE, DD, and NW contributed to the writing process. All authors revised and approved the manuscript.
Handling co-editors: Marianne Westberg and Robin Christensen
Acta thanks Volker Thomas Christian Otten and Christof Wagner for help with peer review of this manuscript.
The goal of orthopedic surgery training programs is to provide operative training for young physicians while continuing safe and efficacious patient care. Training programs have evolved making sure that trainees (residents) are gradually exposed to surgical procedures with increasing complexity. During training, surgical skills are acquired predominantly in the operating room where the resident is supervised by an experienced orthopedic surgeon. Because both the surgeon and resident actively contribute to the operation, every step of the procedure receives attention. Although surgical training is an important part of the residency program, patients may prefer a surgeon with more experience performing the procedure. One of the reasons is the societal concern that resident involvement may result in more adverse events. Our systematic review aims to investigate whether resident involvement is associated with a higher complication rate in total hip and knee arthroplasty (THA/TKA) compared with procedures performed by orthopedic surgeons.
Methods
The systematic literature review regarding the association of resident involvement with complications after THA and TKA was reported according to the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) guidelines [1]. We defined the following PICO question: our population (P) as patients who underwent THA or TKA [2]. The intervention (I) was defined as orthopedic residents involved in the surgical procedure. We compared (C) this intervention with procedures performed by orthopedic surgeons for the outcome (O) all reported complications. Study design (S) consisted of all published literature with the exception of reviews.
Literature search
The protocol was not registered in an international database, which is why we were unable to comply with PRISMA item 24a.
A search strategy was designed supported by a specialist (CdH), to identify relevant publications in PubMed, Embase. com, CENTRAL, Cinahl/Ebscohost, and Web of Science. The search included index terms as well as free text words. Supplementary Table 1 summarizes the full search strategy for all databases. The electronic search was updated on November 2, 2023, searching all databases from inception. Literature in English, German, French, and Dutch was included.
Study selection and data extraction
All manuscripts were included that described: (i) complications in primary THA and/or TKA and (ii) comparing procedures with and without resident involvement. Studies that did not differentiate between procedures with and without resident involvement were excluded. 2 reviewers (DK and NW) independently assessed the literature by screening title and abstract using Rayyan [3]. Subsequently, full-text articles were examined for eligibility. In addition, bibliographies of all included full-text articles were reviewed to identify potential additional eligible articles. During the selection, the reviewers were blinded to each other’s assessment.
Data extraction of the selected manuscripts was performed independently by 2 reviewers (DK and NW) using a predefined data extraction sheet. The original manuscripts were reviewed without blinding for authors and affiliation. Relevant data regarding the country of origin, study type, data source, joint(s) involved, number of patients, follow-up, mortality, and any reported complication was extracted from the text and tables. All complications reported in the study were extracted from the studies. Studies describing summarized complication rates were included in the analysis of the overall and surgical site complication analysis.
Study quality was determined independently by the 2 reviewers using a standardized grading tool (MINORS criteria) [4]. The items were scored 0 if not reported, 1 when reported but inadequate and 2 when reported and adequate. For comparative studies, the scores can be interpreted as 0–6, very low quality; 7–12, low quality; 13–18 fair quality; and 19–24, high quality [5]. Disagreements between reviewers in manuscript selection, data extraction, and grading of study quality were resolved in a consensus meeting. To assess the risk of bias due to missing evidence according to the RoB-ME tool, a cross-check of the methods and results section was done one against the other to identify any outcomes with no or incomplete results reported.
Statistics
A meta-analysis of the studies was performed using Review Manager software (RevMan Version 5.3, Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2008). Risk ratios were calculated to quantify how strongly the mortality and complications were associated with the involvement of residents. For combining the results found in the different trials the statistical method of Mantel–Haenszel with random effects method was used for dichotomous outcomes, and risk ratios for THA and TKA procedures with and without resident involvement were calculated. Heterogeneity between studies was assessed by using I2 statistics. I2 values between 30–60%, 50–90%, and 75–100% represent moderate, substantial, and considerable heterogeneity, respectively [6]. Risk ratios (RR) with 95% confidence intervals (CI) were reported and a P value of < 0.05 was considered statistically significant.
Ethics, data sharing plan, funding, use of AI, and disclosures
For this systematic review, no ethical approval was required. For data-sharing purposes, extracted data is provided in the supplementary files. During this project and the preparation of the manuscript, no artificial intelligence tools were used. No funding was received for this study. The authors declare that they have no conflicts of interest regarding this research. Complete disclosure of interest forms according to ICMJE are available on the article page, doi: 10.2340/17453674.2025.43905
Results
Study selection and data extraction
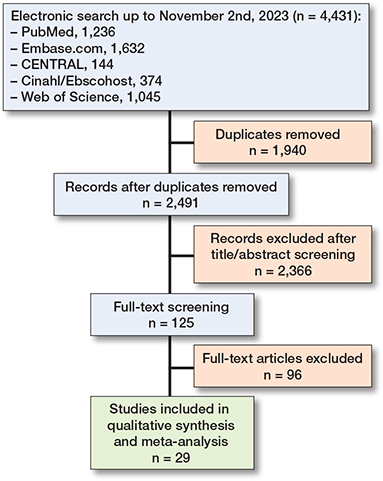
The search strategy yielded 4,431 articles, of which 2,491 remained after deduplication (Figure). Of these studies, 2,366 were excluded after screening of titles and abstracts. After fulltext screening of the remaining 125 articles, 29 articles were included for this review. All excluded articles did not provide data describing complications in populations operated on with or without resident involvement. Cross-referencing did not result in additional studies. 2 prospective and 27 retrospective cohort studies [7-35] were included consisting of 12 examining complications in THA, 12 in TKA, and 5 in both (Table 1). The number of patients ranged from 50 to 89,087 and followup duration between discharge from the ward and 10 years. For the assessment of the risk of bias due to missing evidence no study protocols or pre-specified analysis plans were found for the cohort studies. Although reporting of complications in the methods section was often limited, reporting of the outcome was detailed, and no discrepancies were found when cross-checking the methods and results section. Due to the poor description of complications in the methods section and nature of the studies, selective reporting bias in some studies is likely. The direction of the possible bias is unpredictable. The reporting on outcomes in the methods section and the extracted complications from each study are provided in Supplementary Table S2.
| 1st author | Country | Study type a | Data source b | Joint c | Total | Patients, n Residents | OS | Follow-up | Ref |
| Lederer 2001 | Germany | R | Single center | h | 3,290 | 1,290 | 2,000 | ND | 7 |
| Moran 2004 | UK | P | Single center | h | 536 | 139 | 397 | 1.5 years | 8 |
| Robinson 2007 | USA | R | Single center | h | 135 | 52 | 83 | 1 year | 9 |
| Woolson 2007 | USA | R | Single center | h & k | 401 | 191 | 210 | > 6 months | 10 |
| Palan 2009 | UK | R | Multi-center | h | 1,501 | 528 | 973 | 5 years | 11 |
| Inglis 2012 | New Zealand | R | NZJR 2005-2011 | h | 34,393 | 4,049 | 30,344 | 6 years | 12 |
| Schoenfeld 2013 | USA | R | NSQIP 2005-2010 | h & k | 23,783 | 4,816 | 18,967 | 30 days | 13 |
| Bohl 2014 | USA | R | NSQIP 2006-2010 | h & k | 21,434 | 4,260 | 17,174 | 30 days | 14 |
| Haughom 2014 | USA | R | NSQIP 2005-2012 | h | 13,109 | 3,462 | 9,647 | ND | 15 |
| Haughom 2014 | USA | R | NSQIP 2005-2012 | k | 24,529 | 5,960 | 18,569 | ND | 16 |
| Hasegawa 2015 | Japan | R | Single center | h | 483 | 259 | 224 | 5.1 years | 17 |
| Reidy 2016 | UK | R | Multi-center | h | 870 | 286 | 584 | 10 years | 18 |
| Wilson 2016 | Australia | R | Single center | h & k | 4918 | 2,313 | 2,605 | ND | 19 |
| Faulkner 2017 | UK | R | Multi-center | k | 686 | 236 | 450 | 10 years | 20 |
| Weber 2017 | Germany | R | Single center | h | 1,008 | 240 | 768 | 1 year | 21 |
| Weber 2017 | Germany | R | Single center | k | 738 | 292 | 446 | 1 year | 22 |
| Windisch 2017 | Germany | R | Single center | k | 1,068 | 80 | 988 | 3 years | 23 |
| Beattie 2018 | UK | R | Single center | k | 609 | 144 | 465 | 1 year | 24 |
| Smith 2018 | New Zealand | R | NZJR 2000-2014 | h | 89,087 | 9,586 | 79,501 | 0.5 year | 25 |
| Theelen 2018 | Netherlands | R | Single center | k | 642 | 220 | 422 | 4.5 years | 26 |
| MacDonald 2019 | UK | R | Single center | h | 87 | 44 | 43 | 13 months | 27 |
| Nakamura 2019 | Japan | P | Single center | k | 100 | 58 | 42 | > 3 months | 28 |
| Foissey 2020 | France | R | Single center | h | 488 | 147 | 341 | 3 years | 29 |
| Bron 2021 | Netherlands | R | Multi-center | h & k | 7,123 | 2,027 | 5,096 | > 3 months | 30 |
| Hoerlesberger 2021 | Austria | R | Single center | k | 206 | 103 | 103 | Till discharge | 31 |
| Sheridan 2022 d | Canada | R | Single center | k | 315 | 315 | 315 | >4 years | 32 |
| Maheshwari 2022 d | USA | R | Single center | k | 50 | 50 | 50 | 1 year | 33 |
| Anis 2022 | USA | R | Multi-center | k | 12,664 | 7,234 | 5,430 | 1 year | 34 |
| Stafford 2023 | USA | R | Single center | k | 200 | 100 | 100 | 14 months | 35 |
| a Study type: prospective (P) or retrospective (R) cohort study. b Data source: New Zealand Joint Registry (NZJR) and National Surgical Quality Improvement Program (NSQIP). c h: hip; k: knee. d Bilateral knee replacement (one side consultant, other side resident). ND: no data; OS: orthopedic surgeon. |
|||||||||
The mean MINORS score was 13.7 ranging from 10 to 17 (Table 2). The quality can be interpreted as low in 9 studies and fair in 20 studies. 2 studies used the New Zealand Joint Registry (NZJR) and 4 studies the National Surgical Quality Improvement Program (NSQIP) as the source of their data [12-16,25]. To avoid including overlapping cohorts for some complications, a selection of these studies was made during data analysis. The studies with the highest number of reported complications for hip and knee arthroplasties combined were included in the analysis.
| Study | A | B | C | D | E | F | G | H | I | J | K | L | M |
| Lederer 2001 | 2 | 2 | 0 | 2 | 0 | 0 | 0 | 0 | 2 | 2 | 0 | 1 | 11 |
| Moran 2004 | 1 | 0 | 2 | 1 | 0 | 2 | 1 | 0 | 2 | 2 | 1 | 1 | 13 |
| Robinson 2007 | 2 | 0 | 1 | 1 | 0 | 2 | 1 | 1 | 2 | 2 | 0 | 1 | 13 |
| Woolson 2007 | 1 | 2 | 1 | 2 | 0 | 2 | 0 | 2 | 2 | 2 | 0 | 1 | 15 |
| Palan 2009 | 2 | 0 | 2 | 1 | 0 | 2 | 1 | 0 | 2 | 2 | 0 | 1 | 13 |
| Inglis 2012 | 1 | 0 | 0 | 1 | 0 | 2 | 0 | 0 | 2 | 2 | 0 | 2 | 10 |
| Schoenfeld 2013 | 2 | 0 | 0 | 2 | 0 | 2 | 0 | 0 | 2 | 2 | 0 | 2 | 12 |
| Bohl 2014 | 1 | 0 | 0 | 2 | 0 | 1 | 0 | 0 | 2 | 2 | 0 | 2 | 10 |
| Haughom 2014 | 2 | 0 | 0 | 2 | 0 | 1 | 0 | 0 | 2 | 2 | 1 | 2 | 12 |
| Haughom 2014 | 2 | 0 | 0 | 2 | 0 | 1 | 0 | 0 | 2 | 2 | 1 | 2 | 12 |
| Hasegawa 2015 | 1 | 2 | 2 | 2 | 0 | 2 | 1 | 0 | 2 | 2 | 0 | 1 | 15 |
| Reidy 2016 | 2 | 2 | 0 | 1 | 0 | 2 | 2 | 0 | 2 | 2 | 0 | 2 | 15 |
| Wilson 2016 | 1 | 2 | 2 | 1 | 0 | 2 | 0 | 0 | 2 | 2 | 1 | 1 | 14 |
| Faulkner 2017 | 2 | 2 | 1 | 2 | 0 | 2 | 1 | 0 | 2 | 2 | 1 | 2 | 17 |
| Weber 2017 | 2 | 1 | 1 | 2 | 0 | 2 | 0 | 2 | 2 | 2 | 1 | 1 | 16 |
| Weber 2017 | 2 | 1 | 1 | 2 | 0 | 2 | 0 | 2 | 2 | 2 | 1 | 1 | 16 |
| Windisch 2017 | 2 | 1 | 1 | 2 | 0 | 2 | 0 | 0 | 2 | 2 | 0 | 1 | 13 |
| Beattie 2018 | 2 | 2 | 1 | 1 | 0 | 2 | 0 | 0 | 2 | 2 | 2 | 1 | 15 |
| Smith 2018 | 2 | 0 | 0 | 1 | 0 | 2 | 0 | 0 | 2 | 2 | 1 | 1 | 11 |
| Theelen 2018 | 2 | 1 | 0 | 1 | 0 | 2 | 0 | 0 | 2 | 2 | 2 | 1 | 13 |
| MacDonald 2019 | 2 | 2 | 1 | 2 | 0 | 1 | 0 | 0 | 2 | 2 | 0 | 0 | 12 |
| Nakamura 2019 | 1 | 2 | 2 | 1 | 0 | 1 | 2 | 0 | 2 | 2 | 2 | 1 | 16 |
| Foissey 2020 | 2 | 1 | 1 | 1 | 0 | 2 | 2 | 0 | 2 | 2 | 1 | 1 | 15 |
| Bron 2021 | 2 | 2 | 1 | 2 | 0 | 2 | 0 | 0 | 2 | 2 | 1 | 2 | 16 |
| Hoerlesberger 2021 | 2 | 1 | 0 | 1 | 0 | 0 | 0 | 2 | 2 | 2 | 1 | 1 | 12 |
| Sheridan 2022 | 2 | 1 | 0 | 1 | 0 | 2 | 1 | 0 | 2 | 2 | 2 | 2 | 15 |
| Maheshwari 2022 | 1 | 1 | 0 | 1 | 1 | 1 | 2 | 0 | 2 | 2 | 2 | 2 | 15 |
| Anis 2022 | 2 | 2 | 0 | 1 | 0 | 1 | 2 | 0 | 2 | 2 | 1 | 2 | 15 |
| Stafford 2023 | 2 | 2 | 0 | 2 | 0 | 1 | 2 | 0 | 2 | 1 | 2 | 1 | 15 |
| A Clearly stated aim B Inclusion of consecutive patients C Prospective collection of data D Endpoint appropriate to study aim E Unbiased assessment of endpoints F Follow-up appropriate to study aim G < 5% loss to follow-up H Prospective calculation of study size I Adequate control group J Contemporary groups K Baseline equivalance of groups L Adequate statistical analysis M Total |
|||||||||||||
Overall complication rate and mortality
9 (n = 51,442) and 12 (n = 37,789) studies were included in the analysis of the overall and surgical complication rate, respectively. Although there was substantial heterogeneity, pooled data showed that resident involvement was not significantly associated with a higher overall or surgical complication rate compared with procedures performed by an orthopedic surgeon (Table 3 and Supplementary Forest plots S3 A–B). Comparison of the mortality was performed in 6 studies (n = 32,768) and showed no significant association of the involvement of residents with early death (< 90 days) (Supplementary Forest plot S3 C).
Surgical site complications
Of the investigated complications, deep infection could be associated with resident involvement (RR 1.55, CI 1.09–2.20): 193 of 27,170 (0.7%) of the cases with a resident involved developed a deep infection compared with 342 of 116,053 (0.3%) cases without resident involvement (Table 4 and Supplementary Forest plot S4A). Although there was heterogeneity for some of the complications, none of the other surgical complications (reoperation, THA dislocation, fracture, nerve palsy, superficial infection, aseptic loosening, limited mobility of TKAs, instability of TKAs, wound defect, malalignment of TKAs, serious drainage/hematoma, wound complications [not specified], acetabular perforations, blistering, patellar dislocation in TKAs, psoas pain/impingement, arterial injury subluxations, insert wear in TKAs, patellar wear, heterotopic ossifications, and patellar clunk) could be associated with resident involvement (Table 4 and Supplementary Forest plots S4 B–L). Pooling of the data on aseptic loosening bordered the significance level set for this meta-analysis (P = 0.08, Supplementary Forest plot S4 G).
| Complication | Studies (n) | Residents (n/N) | Orthopedic surgeon (n/N) | RR (CI) | P value | I2 (%) |
| Overall complications | 9 | 1,549/14,428 | 3,007/37,014 | 1.07 (0.97-1.19) | 0.2 | 46 |
| Deep infection | 18 | 193/27,170 | 342/116,053 | 1.55 (1.09-2.20) | 0.01 | 48 |
| Reoperation | 14 | 269/17,684 | 890/68,379 | 1.11 (0.92-1.34) | 0.3 | 17 |
| Dislocation THA | 12 | 113/8,304 | 304/38,746 | 1.17 (0.94-1.46) | 0.2 | 0 |
| Fracture | 9 | 33/6,843 | 119/35,180 | 0.90 (0.59-1.37) | 0.6 | 0 |
| Nerve palsy | 9 | 64/9,222 | 102/27,690 | 1.42 (0.83-2.43) | 0.2 | 39 |
| Superficial infection | 7 | 264/17,244 | 376/35,589 | 0.99 (0.84-1.17) | 0.9 | 0 |
| Aseptic loosening | 7 | 24/5,209 | 95/32,372 | 1.50 (0.95-2.37) | 0.08 | 0 |
| Limited mobility TKA | 5 | 17/893 | 14/1,336 | 1.60 (0.80-3.21) | 0.2 | 0 |
| Instability TKA | 2 | 2/316 | 5/1,438 | 2.18 (0.08-58.95) | 0.6 | 72 |
| Wound defect | 4 | 23/9,901 | 56/28,862 | 1.21 (0.74-1.98) | 0.5 | 0 |
| Malalignment TKA | 2 | 0/308 | 4/549 | 0.32 (0.04-2.74) | 0.3 | 0 |
| Serious drainage/hematoma | 2 | 5/243 | 3/293 | 1.81 (0.47-6.94) | 0.4 | 0 |
| Wound complication a | 1 | 160/2,313 | 175/2,605 | 1.03 (0.84-1.27) | 0.8 | NA |
| Acetabular perforations | 1 | 9/1,290 | 10/2,000 | 1.40 (0.57-3.42) | 0.5 | NA |
| Blistering | 1 | 0/220 | 3/422 | 0.27 (0.01-5.27) | 0.4 | NA |
| Patellar dislocation TKA | 1 | 0/220 | 2/422 | 0.38 (0.02-7.94) | 0.5 | NA |
| Psoas pain/impingement | 1 | 4/147 | 18/341 | 0.52 (0.18-1.50) | 0.2 | NA |
| Gluteus tendinitis | 1 | 2/147 | 8/341 | 0.58 (0.12-2.70) | 0.5 | NA |
| Arterial injury | 1 | 2/259 | 0/224 | 4.33 (0.21-90) | 0.3 | NA |
| Subluxations | 1 | 4/191 | 1/210 | 4.40 (0.50-39) | 0.2 | NA |
| Insert wear TKA | 1 | 0/191 | 1/210 | 0.37 (0.02-8.94) | 0.5 | NA |
| Patellar wear | 1 | 1/191 | 1/210 | 1.10 (0.07-17) | 0.9 | NA |
| Heterotopic ossifications | 1 | 3/119 | 0/111 | 6.53 (0.34-125) | 0.2 | NA |
| Patellar clunk | 1 | 0/50 | 1/50 | 0.33 (0.01-7.99) | 0.5 | NA |
| CI: 95% confidence interval; TKA: total knee arthroplasty; NA: not applicable. See supplementary forest plot files for details. a Unspecified. |
||||||
Systemic complications
None of the thrombo-embolic, pulmonary, cardiac, neurological, or gastrointestinal complications were associated with involvement of residents during total knee and/or hip arthroplasty. Only any urological complications (RR 1.52, CI 1.17–1.96) and sepsis (RR 1.80 CI 1.22–2.65) happened significantly more when a resident was involved (Table 5 and Supplementary Forest plots S5 A–L).
| Complication | Studies (n) | Residents (n/N) | Orthopedic surgeon (n/N) | RR (CI) | I2 P value | (%) |
| Pulmonary a | ||||||
| On ventilator > 48 h | 2 | 12/9,422 | 20/28,216 | 1.79 (0.88-3.64) | 0.1 | 37 |
| Unplanned intubation | 2 | 19/9,422 | 59/28,216 | 0.96 (0.57-1.61) | 0.9 | 42 |
| Pneumonia | 2 | 35/9,422 | 100/28,216 | 0.88 (0.29-2.70) | 0.8 | 83 |
| Any pulmonary compl. | 1 | 14/2,027 | 34/5,096 | 1.04 (0.56-1.92) | 0.9 | NA |
| Cardiac | ||||||
| Cardiac arrest | 2 | 6/9,422 | 27/28,216 | 0.70 (0.29-1.71) | 0.4 | 0 |
| Myocardial infarction | 2 | 29/9,422 | 61/28,216 | 1.44 (0.92-2.23) | 0.1 | 0 |
| Any cardiac compl. | 1 | 35/2,027 | 68/5,096 | 1.29 (0.86-1.94) | 0.2 | NA |
| Hypotension | 1 | 3/220 | 1/422 | 5.75 (0.60-55) | 0.1 | NA |
| Hypovolemic shock | 1 | 1/220 | 0/422 | 5.74 (0.23-140) | 0.3 | NA |
| Cardiac arrythmia | 1 | 1/220 | 0/422 | 5.74 (0.23-140) | 0.3 | NA |
| Thrombo-embolic | ||||||
| Deep venous thrombosis | 6 | 126/11,106 | 289/30,795 | 1.17 (0.95-1.44) | 0.2 | 0 |
| Pulmonary embolism | 6 | 74/11,220 | 169/31,171 | 1.21 (0.87-1.68) | 0.3 | 10 |
| Neurological | ||||||
| Cerebrovascular accident | 3 | 14/11,449 | 48/33,312 | 0.85 (0.46-1.54) | 0.6 | 0 |
| Delirium | 1 | 41/2,027 | 78/5,096 | 1.32 (0.91-1.92) | 0.1 | NA |
| Coma | 1 | 1/4,260 | 0/17,174 | 12.1 (0.49-296) | 0.1 | NA |
| Renal/Urological | ||||||
| Renal insufficiency | 2 | 8/,422 | 37/28,216 | 0.66 (0.31-1.43) | 0.3 | 0 |
| Acute renal failure | 2 | 5/9,422 | 29/28,216 | 0.52 (0.20-1.35) | 0.2 | 0 |
| Urinary tract infection | 2 | 144/9,422 | 401/28,216 | 1.07 (0.89-1.30) | 0.5 | 0 |
| Any urologic compl. | 1 | 90/2,027 | 149/5,096 | 1.52 (1.17-1.96) | 0.001 | NA |
| Gastrointestinal | 1 | 10/2,027 | 21/5,096 | 1.20 (0.56-2.54) | 0.6 | NA |
| Infectious | ||||||
| Sepsis | 1 | 37/4,816 | 81/18,967 | 1.80 (1.22-2.65) | 0.003 | NA |
| Septic shock | 1 | 4/4,816 | 29/18,967 | 0.54 (0.19-1.54) | 0.3 | NA |
| Organ infection | 1 | 7/4,260 | 23/17,174 | 1.23 (0.53-2.86) | 0.6 | NA |
| Unplanned readmission | 2 | 92/9,422 | 230/28,216 | 1.20 (0.94-1.53) | 0.1 | NA |
| a Pulmonary embolism excluded. NA: not applicable. See supplementary forest plot files for details. | ||||||
Discussion
We aimed to investigate the association between resident involvement and complication rate in total hip and knee arthroplasty and showed no significant association with overall complications, overall surgical complications, or mortality. For each of the individually reported surgical complications, a significant association was found only for resident involvement and deep infection. For the individual systemic complications, resident involvement was associated with a significant difference for any urologic complications and sepsis but only based on 2 studies [13,30]. Overall, these results imply that our current way of training orthopedic surgeon may expose patients to a slight increased infection risk for complications during total joint arthroplasty.
In contrast to previous reviews, this is the first report finding an association between resident involvement and deep infection [36-38]. The increased infection risk may be explained by increased surgical time in trainee involved procedures [9,11,21,34,37-39]. Increased surgical time has proven in multiple studies to be an independent risk factor for infection in total joint arthroplasty [40-43]. In a recent study, resident involvement did not independently increase the risk for infection. However, cases with resident involvement were associated with longer operative times and patients with increased medical complexity, both of which were found to be independently associated with an increased risk of infection [34]. It could very well be that there is a logical longer duration of the procedure due to “teaching time,” which may have increased infection risk [44-47]. However, this does not result in a higher number of other complications.
Limitations
Due to the nature of the retrospective cohort studies, non-reporting of risk factors and reporting bias are likely present in some studies. Furthermore, selection bias will also be likely in these studies as complex patients with higher infection risks are more often treated in large teaching hospitals instead of smaller private clinics without resident training programs. Low surgeon volume and prolonged duration of the surgical procedure are also mentioned as risk factors. Naturally, the exposure of residents to high volumes of total joint arthroplasty is still limited during their training. Another limitation could be the heterogeneity within training programs because trainees receive different kinds of responsibilities and independence in the operating theatre according to their progression and number of years in training.
Clinical implications
Although there are no guidelines stating which differences in risk ratio for complications are acceptable or clinically important, deep infection is one of the most serious complications in total joint arthroplasty and the risk should be minimized. We suggest that training programs should be alert to time, so that thresholds for increased infection risks are not overrun. Each procedure should be divided into different parts or steps and given a maximum duration. If the trainee exceeds this time, the consultant or supervisor should take over. These parts of the surgery can also be allocated to trainee or consultant before the start of the procedure to put more focus on the learning objective for the specific procedure.
Conclusion
We showed no evidence of an association between resident involvement and more overall or surgical site complications in primary TKAs and THAs compared with orthopedic surgeons. However, resident involvement was associated with a higher risk of deep infection, any urologic complications, and sepsis.
In perspective, it is recommended to be alert to the training time and maximum duration of the surgical procedure. This can help teaching hospitals to improve the resident training program and may help to reassure patients.
Supplementary data
Search terms, reported complications per article, and Tables with forest plots of complications are available as Supplementary data on the article page, doi: 10.2340/17453674.2025.43905
- Page M J, McKenzie J E, Bossuyt P M, Boutron I, Hoffmann T C, Mulrow C D, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ 2021; 372:n71. doi: 10.1136/bmj.n71.
- Richardson W S, Wilson M C, Nishikawa J, Hayward R S. The well-built clinical question: a key to evidence-based decisions. ACP J Club 1995; 123(3): A12-13. NOT CITED
- Ouzzani M, Hammady H, Fedorowicz Z, Elmagarmid A. Rayyan: a web and mobile app for systematic reviews. Syst Rev 2016; 5(1): 210. doi: 10.1186/s13643-016-0384-4.
- Slim K, Nini E, Forestier D, Kwiatkowski F, Panis Y, Chipponi J. Methodological index for non-randomized studies (MINORS): development and validation of a new instrument. ANZ J Surg 2003; 73(9): 712-16. doi: 10.1046/j.1445-2197.2003.02748.x.
- Khan W, Khan M, Alradwan H, Williams R, Simunovic N, Ayeni O R. Utility of intra-articular hip injections for femoroacetabular impingement: a systematic review. Orthop J Sports Med 2015; 3(9): 2325967115601030. doi: 10.1177/2325967115601030.
- Deeks J J, Higgins J P T, Altman D G. Chapter 9: Analysing data and undertaking meta-analyses. In: Higgins J P T, Green S, editors. Cochrane Handbook for Systematic Reviews of Interventions 510. The Cochrane Collaboration, 2011 ed; 2011. p. Available from www.cochrane-handbook.org
- Lederer M, Muller R T. [Effect of graduate education on complication rate and costs of hip prosthesis implantation]. Unfallchirurg 2001; 104(7): 577-82. doi: 10.1007/s001130170088.
- Moran M, Yap S L, Walmsley P, Brenkel I J. Clinical and radiologic outcome of total hip arthroplasty performed by trainee compared with consultant orthopedic surgeons. J Arthroplasty 2004; 19(7): 853-7. doi: 10.1016/j.arth.2004.06.026.
- Robinson R P. The impact of resident teaching on total hip arthroplasty. Clin Orthop Relat Res 2007; 465: 196-201. doi: 10.1097/BLO.0b013e3181576006.
- Woolson S T, Kang M N. A comparison of the results of total hip and knee arthroplasty performed on a teaching service or a private practice service. J Bone Joint Surg Am 2007; 89(3): 601-7. doi: 10.2106/JBJS.F.00584.
- Palan J, Gulati A, Andrew J G, Murray D W, Beard D J. The trainer, the trainee and the surgeons’ assistant: clinical outcomes following total hip replacement. J Bone Joint Surg Br 2009; 91(7): 928-34. doi: 10.1302/0301-620X.91B7.22021
- Inglis T, Dalzell K, Hooper G, Rothwell A, Frampton C. Does orthopedic training compromise the outcome in total hip arthroplasty? J Surg Educ 2013; 70(1): 76-80. doi: 10.1016/j.surg.2012.08.003.
- Schoenfeld A J, Serrano J A, Waterman B R, Bader J O, Belmont P J Jr. The impact of resident involvement on post-operative morbidity and mortality following orthopaedic procedures: a study of 43,343 cases. Arch Orthop Trauma Surg 2013; 133(11): 1483-91. doi: 10.1007/s00402-013-1841-3.
- Bohl D D, Fu M C, Golinvaux N S, Basques B A, Gruskay J A, Grauer J N. The “July effect” in primary total hip and knee arthroplasty: analysis of 21,434 cases from the ACS-NSQIP database. J Arthroplasty 2014; 29(7): 1332-8. doi: 10.1016/j.arth.2014.02.008.
- Haughom B D, Schairer W W, Hellman M D, Yi P H, Levine B R. Resident involvement does not influence complication after total hip arthroplasty: an analysis of 13,109 cases. J Arthroplasty 2014; 29(10): 1919-24. doi: 10.1016/j.arth.2014.06.003.
- Haughom B D, Schairer W W, Hellman M D, Yi P H, Levine B R. Does resident involvement impact post-operative complications following primary total knee arthroplasty? An analysis of 24,529 cases. J Arthroplasty 2014; 29(7): 1468-72.e2. doi: 10.1016/j.arth.2014.02.036.
- Hasegawa Y, Amano T. Surgical skills training for primary total hip arthroplasty. Nagoya J Med Sci 2015; 77(1-2): 51-7.
- Reidy M J, Faulkner A, Shitole B, Clift B. Do trainee surgeons have an adverse effect on the outcome after total hip arthroplasty?: a tenyear review. Bone Joint J 2016; 98-B(3): 301-6. doi: 10.1302/0301-620X.98B3.35997.
- Wilson M D, Dowsey M M, Spelman T, Choong P F. Impact of surgical experience on outcomes in total joint arthroplasties. ANZ J Surg 2016; 86(12): 967-72. doi: 10.1111/ans.13513.
- Faulkner A, Reidy M J, Davies P S E, Wang W, Buddhadev N, Johnston L, et al. Balancing training and outcomes in total knee replacement: a ten-year review. Surgeon 2018; 16(4): 227-31. doi: 10.1016/j.surge.2017.10.003.
- Weber M, Benditz A, Woerner M, Weber D, Grifka J, Renkawitz T. Trainee surgeons affect operative time but not outcome in minimally invasive total hip arthroplasty. Sci Rep 2017; 7(1): 6152. doi: 10.1038/s41598-017-06530-3.
- Weber M, Worlicek M, Voellner F, Woerner M, Benditz A, Weber D, et al. Surgical training does not affect operative time and outcome in total knee arthroplasty. PloS One 2018; 13(6): e0197850. doi: 10.1371/journal.pone.0197850.
- Windisch C, Brodt S, Rohner E, Matziolis G. [Complications and costs in primary knee replacement surgery in an endoprosthetics centre: influence of state of training]. Orthopade 2017; 46(4): 353-8. doi: 10.1007/s00132-016-3351-9.
- Beattie N, Maempel J F, Roberts S, Waterson H B, Brown G, Brenkel I J, et al. Surgery performed by supervised registrars does not adversely affect medium-term functional outcomes after total knee replacement. AnnR Coll Surg Engl 2018; 100(1): 57-62. doi: 10.1308/rcsann.2017.0164.
- Smith J O, Frampton C M A, Hooper G J, Young S W. The impact of patient and surgical factors on the rate of postoperative infection after total hip arthroplasty: a New Zealand Joint Registry study. J Arthroplasty 2018; 33(6): 1884-90. doi: 10.1016/j.arth.2018.01.021.
- Theelen L, Bischoff C, Grimm B, Heyligers I C. Current practice of orthopaedic surgical skills training raises performance of supervised residents in total knee arthroplasty to levels equal to those of orthopaedic surgeons. Perspect Med Educ 2018; 7(2): 126-32. doi: 10.1007/s40037-018-0408-y.
- MacDonald D R W, Dougall T W, Mitchell M, Farrow L. Can total hip arthroplasty for hip fracture be safely performed by trainees? A retrospective cohort study. J Arthroplasty 2020; 35(5): 1303-6. doi: 10.1016/j.arth.2019.12.030.
- Nakamura J, Shimizu K, Suguro T, Hagiwara S, Orita S, Akazawa T, et al. Direct medial approach for primary total knee arthroplasty: preliminary results of a novel surgical technique. Chiba Med J 2019; 95E:45-52.
- Foissey C, Fauvernier M, Fary C, Servien E, Lustig S, Batailler C. Total hip arthroplasty performed by direct anterior approach: does experience influence the learning curve? SICOT J 2020; 6:15. doi: 10.1051/sicotj/2020015.
- Bron D, Wolterbeek N, Poolman R, Kempen D, Delawi D. Resident training does not influence the complication risk in total knee and hip arthroplasty. Acta Orthop 2021: 1-6. doi: 10.1080/17453674.2021.1979296.
- Hoerlesberger N, Glehr M, Amerstorfer F, Hauer G, Leithner A, Sadoghi P. Residents’ learning curve of total knee arthroplasty based on radiological outcome parameters: a retrospective comparative study. J Arthroplasty 2021; 36(1): 154-9. doi: 10.1016/j.arth.2020.07.045.
- Sheridan G A, Moshkovitz R, Masri B A. Simultaneous bilateral total knee arthroplasty: similar outcomes for trainees and trainers. Bone Jt Open 2022; 3(1): 29-34. doi: 10.1302/2633-1462.31.BJO-2021-0186.R1.
- Maheshwari A V, Garnett C T, Cheng T H, Buksbaum J R, Singh V, Shah N V. Does resident participation influence surgical time and clinical outcomes? An analysis on primary bilateral single-staged sequential total knee arthroplasty. Arthroplast Today 2022; 15: 202-9.e4. doi: 10.1016/j.artd.2022.02.029.
- Anis H K, Rothfusz C A, Eskildsen S M, Klika A K, Piuzzi N S, Higuera C A, et al. Does surgical trainee participation affect infection outcomes in primary total knee arthroplasty? J Surg Educ 2022; 79(4): 993-9. doi: 10.1016/j.surg.2022.02.006.
- Stafford J A, DeVito P, Grewal G, Davis T A, Guerra C, Corces A. Resident impact on primary total knee arthroplasty: a consecutive series under a single surgeon. Arthroplast Today 2023; 23:101175. doi: 10.1016/jartd.2023.101175.
- Madanipour S, Singh P, Karia M, Bhamra J S, Abdul-Jabar H B. Trainee performed total knee arthroplasty is safe and effective: a systematic review and meta-analysis comparing outcomes between trainees and consultants. Knee 2021; 30: 291-304. doi: 10.1016/j.knee.2021.04.013.
- Marder R S, Gopie I, Ikwuazom C P, Tozzi D, Shah N V, Naziri Q, et al. The impact of surgical trainee involvement in total hip arthroplasty: a systematic review of surgical efficacy, patient safety, and outcomes. Eur J Orthop Surg Traumatol 2023; 33(4): 1365-409. doi: 10.1007/s00590-022-03290-3.
- Singh P, Madanipour S, Fontalis A, Bhamra J S, Abdul-Jabar H B. A systematic review and meta-analysis of trainee- versus consultant surgeon-performed elective total hip arthroplasty. EFORT Open Rev 2019; 4(2): 44-55. doi: 10.1302/2058-5241.4.180034.
- Storey R, Frampton C, Kieser D, Ailabouni R, Hooper G. Does orthopaedic training compromise the outcome in knee joint arthroplasty? J Surg Educ 2018; 75(5): 1292-8. doi: 10.1016/j.surg.2018.02.011.
- Coello R, Charlett A, Wilson J, Ward V, Pearson A, Borriello P. Adverse impact of surgical site infections in English hospitals. J Hosp Infect 2005; 60(2): 93-103. doi: 10.1016/j.jhin.2004.10.019.
- Kunutsor S K, Whitehouse M R, Blom A W, Beswick A D, Team I. Patient-related risk factors for periprosthetic joint infection after total joint arthroplasty: a systematic review and meta-analysis. PloS One 2016; 11(3): e0150866. doi: 10.1371/journal.pone.0150866.
- Song K H, Kim E S, Kim Y K, Jin H Y, Jeong S Y, Kwak Y G, et al. Differences in the risk factors for surgical site infection between total hip arthroplasty and total knee arthroplasty in the Korean Nosocomial Infections Surveillance System (KONIS). Infect Control Hosp Epidemiol 2012; 33(11): 1086-93. doi: 10.1086/668020.
- Triantafyllopoulos G, Stundner O, Memtsoudis S, Poultsides L A. Patient, surgery, and hospital related risk factors for surgical site infections following total hip arthroplasty. Sci World J 2015; 2015: 979560. doi: 10.1155/2015/979560.
- Belmont P J Jr, Goodman G P, Waterman B R, Bader J O, Schoenfeld A J. Thirty-day postoperative complications and mortality following total knee arthroplasty: incidence and risk factors among a national sample of 15,321 patients. J Bone Joint Surg Am 2014; 96(1): 20-6. doi: 10.2106/JBJS.M.00018.
- Duchman K R, Pugely A J, Martin C T, Gao Y, Bedard N A, Callaghan J J. Operative time affects short-term complications in total joint arthroplasty. J Arthroplasty 2017; 32(4): 1285-91. doi: 10.1016/j.arth.2016.12.003.
- Morcos M W, Nowak L, Schemitsch E. Prolonged surgical time increases the odds of complications following total knee arthroplasty. Can J Surg 2021; 64(3): E273-E9. doi: 10.1503/cjs.002720.
- Nowak L L, Schemitsch E H. Duration of surgery affects the risk of complications following total hip arthroplasty. Bone Joint J 2019; 101-B(6_ Supple_B): 51-6. doi: 10.1302/0301-620X.101B6.BJJ-2018-1400.R1.