Comparing incomplete atypical femur fractures in patients with or without bisphosphonate treatment: radiography and bone morphology in a retrospective study of 19 cases
Georg ZDOLSEK 1, Hans Peter BÖGL 2-4, Rickard SAND 1, Aneta LISZKA 3, Anna FAHLGREN 3, and Jörg SCHILCHER 1,5
1 Department of Orthopedic Surgery and Department of Biomedical and Clinical Sciences, Faculty of Health Science, Linköping University, Linköping; 2 Department of Orthopedic Surgery, Gävle Hospital, Gävle; 3 Department of Biomedical and Clinical Sciences, Division of Cell Biology, Linköping University, Linköping; 4 Center for Research and Development, Region Gävleborg/Uppsala University, Gävle; 5 Wallenberg Center for Molecular Medicine, Linköping University, Linköping, Sweden
Background and purpose — Atypical femur fractures (AFF) are associated with bisphosphonate (BP) treatment, although 10–50% of AFF patients have never used BPs. We aimed to compare the medical history, radiographs, and bone biopsies from the fracture site of patients with AFF with (BP group) and without BP exposure (non-BP group).
Methods — Between 2008 and 2021, we included 19 patients aged ≥ 50 years with incomplete AFF. During prophylactic nailing for thigh pain, a biopsy was taken that included the visible fracture line. Medical charts and radiographs were reviewed, and biopsies were analyzed histologically.
Results — In the non-BP group (n = 9; mean age 70 years) patients had diseases affecting bone tissue properties (n = 3), pathological structural variations of the femur geometry or a fatigue-type mechanism (n = 3), or no identified causative patho-mechanism (n = 3). In the BP group (n = 10; mean age, 77 years) 2 patients had pathological variations of femur geometry and all used BPs. In the non-BP group, the fracture line was surrounded by bone resorption (n = 6) and cortical irregularities (n = 3), while the fracture line was restricted to a well-defined line in all patients in the BP group. The bone volume fraction (BV/TV) was on average 18% lower (95% confidence interval –35 to –1.2) in the non-BP group.
Conclusion — AFF in the non-BP group are associated with bone metabolic diseases or deviations in whole-bone geometry and have a specific radiographic appearance at the fracture site whereas antiresorptive treatment appears to be the predominant etiological factor in the BP group.
Citation: Acta Orthopaedica 2025; 96: 421–428. DOI: https://doi.org/10.2340/17453674.2025.43899.
Copyright: © 2025 The Author(s). Published by MJS Publishing – Medical Journals Sweden, on behalf of the Nordic Orthopedic Federation. This is an Open Access article distributed under the terms of the Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0/)
Submitted: 2024-06-12. Accepted: 2025-05-06. Published: 2025-06-05.
Correspondence: jorg.schilcher@liu.se
Study design: JS, GZ, AF, data collection: GZ, JS, AL, data analysis and interpretation: JS, GZ, HPB, manuscript preparation: all authors.
Handling co-editor: Taco Gosens
Acta thanks Hannu T Aro and other anonymous reviewers for help with peer review of this manuscript.
Bisphosphonate (BP) treatment has shown promising results in treating elderly people who have a high risk of fragility fractures. However, acceptance of these drugs has declined because of reports of atypical femur fractures (AFF) being linked to long-term BP use. Several pathophysiological mechanisms for the development of AFF have been proposed, including: femoral geometry influencing stress/strain along the femur; changes in bone matrix composition affecting the mechanical behavior of bone tissue; and suppressed targeted remodeling, leading to the accumulation of microdamage [1]. Only some of the proposed mechanisms are unique to patients who are receiving BP treatment. As AFF also occur in patients who are not receiving BP treatment [2-5], commonly observed principles of stress fracture formation might apply, including: stress beyond the adaptive threshold of the bone tissue with normal elastic resistance (fatigue-type mechanism) [6]; defective elastic resistance due to inherited or acquired changes in bone material properties (insufficiency-type mechanism) [7]; and pathological structural variations of the femur geometry, leading to increased mechanical stress in certain areas of the femur [8] (Table 1, see Appendix).
AFF in patients without BP treatment are very rare (incidence 1/100,000), which makes them difficult to study [5,9]. AFF in BP-treated patients are strongly related to the decreased osteoclast activity characteristic of long-term BP treatment [10], and this reduced osteoclast activity may impact not only bone remodeling, but also the healing mechanisms for incomplete stress fractures and their appearances in radiography, computed tomography (CT), and histology [11].
We aimed to investigate the differences between AFF patients with and without BP treatment through studying the patients’ data, radiographs, and bone biopsies from the fracture site.
Methods
Study design
This retrospective study was performed at the Department of Orthopedic Surgery and the Department of Biomedical and Clinical Sciences, Faculty of Health Science, Linköping University, Sweden between 2008 and 2021. Inclusion criteria were men and women, 50 years or older with an incomplete AFF in need of surgical fixation (Figure 1).
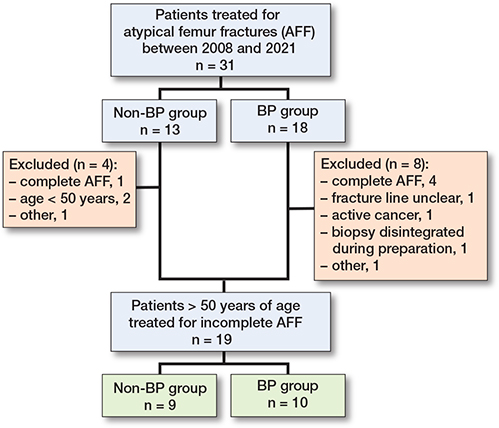
Figure 1. Flowchart describing recruitment to the study cohort. BP = bisphosphonate.
The study is reported according to the STROBE guidelines.
Patients: collection of radiographs and bone biopsies
The patients’ characteristics, drug treatment regimens, and previous diagnoses were obtained through structured medical chart reviews. In addition, standardized patient interviews to identify diagnoses that were linked to an increased risk of stress fractures were performed before study inclusion (Table 2 and Tables S1 and S2, see Supplementary data). During the fracture fixation procedure, all the patients underwent an open bone biopsy that included the visible stress fracture lesion (Figure 2). Endocrinologic consultations were performed either before or after surgery, contingent upon the urgency of the surgical stabilization.
| Item | Non-BP group (n = 9 a) | BP group (n = 10 b) |
| Mean age in years (SD) | 70 (12) | 77 (11) |
| Women | 5 | 9 |
| Treatment with BP for osteoporosis | 0 c | 10 |
| Treatment duration in years (SD) | 0 | 6.7 (5.1) |
| range | 2–21 | |
| Fracture localization | ||
| Shaft (subtrochanteric) | 6 (3) | 9 (1) |
| Bilateral AFF | 2 | 3 |
| Multiple lesions | 4 | 2 |
| Type of treatment | ||
| intramedullary nail d | 6 | 9 |
| dynamic hip screw | 2 | 0 |
| locking plate | 1 | 1 |
| Potential pathologic mechanism | ||
| Paget’s disease of bone | 1 | |
| adynamic bone disease | 1 | |
| hypophosphatemia | 1 | |
| severe coxa vara | 1 | |
| extensive lateral bowing | 1 | |
| heavy loading | 1 e | |
| unspecified | 3 | |
| bisphosphonates | – | 10 |
| extensive lateral and AP | ||
| bowing and coxa vara | – | 2 |
| a 1 case previously published. b 3 cases that have previously been published. c 1 patient received a single dose of Aclasta for Paget’s disease of bone. d All nails included the femoral head in the fixation. e Experienced leg pain after a period of changed working conditions.BP = bisphosphonate; AFF = atypical femur fracture; SD = standard deviation |
||

Figure 2. Biopsy preparation. A. Incomplete AFF. B. Cylindrical cortical defect after the biopsy. C. Cylindrical biopsies cut longitudinal with the fracture line. D. Plane of sectioning.
Definition of AFF and radiographic analyses
AFF were defined according to the 2014 American Society for Bone and Mineral Research (ASBMR) task force major criteria. No or minimal trauma, a transverse fracture line in the lateral femoral cortex below the lesser trochanter and above the supracondylar flare, and focal cortical thickening (callus reaction) were all compulsory in our classification of AFF [12,13] (Figure 3).
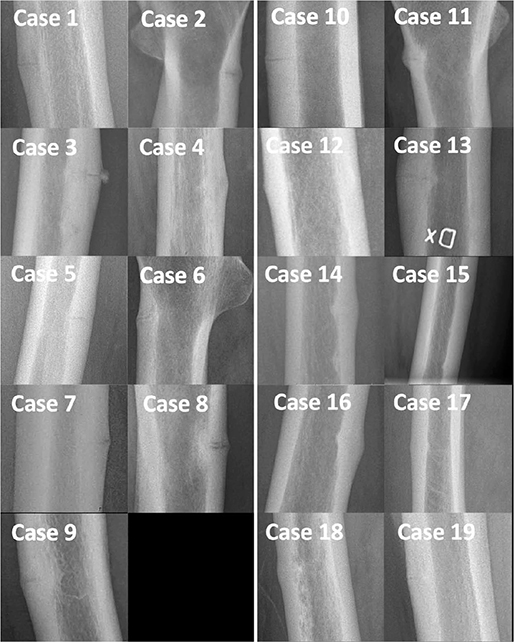
Figure 3. Plain radiographs with magnification at the fracture site. Note the areas of bone resorption and cortical irregularities in the patients in the non-BP group (left panel). In the BP group (right panel) the fracture line was restricted to a well-defined line or no visible fracture line on plain radiographs. BP = bisphosphonate.
Radiographic analyses were performed on standard 2-dimensional preoperative ipsilateral radiographs (Sectra IDS7 OrthoStation; Sectra AB, Linköping, Sweden). The CCD angle (neck–shaft angle) was calculated as the angle between the femoral shaft and the femoral head and neck [14]. Lateral femoral bowing was approximated on standard anteroposterior radiographs [15], and the anterior bowing angle was assessed on lateral view radiographs [16].
We defined subtrochanteric fractures as fractures located < 5 cm below the lesser trochanter, and diaphyseal fractures as fractures located > 5 cm below the lesser trochanter but above the supracondylar flare. The number of fracture lesions was determined on all available radiographs (Figure 4). Contralateral imaging was performed in all patients, to identify possible bilateral fractures.
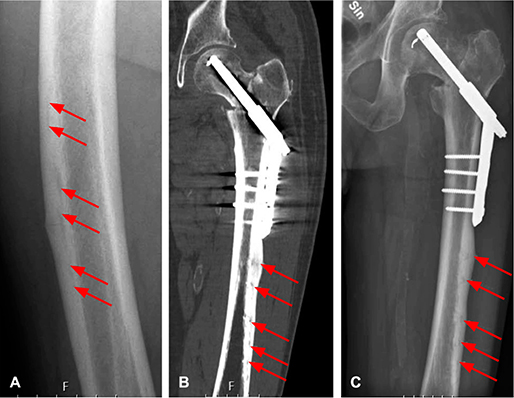
Figure 4. A. Cortical irregularities in proximity to mid-shaft incomplete atypical femur fracture; in Case 1. B and C. Case 3 was treated with a dynamic hip screw plate for an intertrochanteric femur fracture. On the postoperative radiograph, multiple cortical lesions are evident.
Surgery
During prophylactic fixation surgery for fractures, a biopsy that included the fracture line was taken using a cylindrical drill (diameter, 11.5 mm; Diamond TwInS; Karl Storz GmbH, Tuttlingen, Germany). Bone biopsies were fixed in 4% formaldehyde for up to 1 week and then stored in 70% alcohol. The cortical defect that resulted from the biopsy (see Figure 2) allowed the assessment of bone formation during clinical follow-up (Figure S1, see Supplementary data).
Micro-CT
Micro-CT imaging of the bone biopsies was performed postoperatively using the SkyScan 1174 micro-CT (Bruker, Kontich, Belgium). Scans were performed at an angle of 180° with a voltage of 50 kV and using a 1-mm aluminum filter. A rotation step of 0.5°, with a frame averaging of 3 and an image pixel size of 14 μm or 16 μm was used. Reconstructions were carried out with the NRecon software (SkyScan 1174; https://www.bruker.com/en.html); beam hardening of 50% and ring artifact reduction were applied. The micro-CT data was assessed for bone volume fraction (bone tissue volume in relation to all tissue volume; BV/TV) and bone surface density (BS/TV), as well as trabecular thickness (Tb.Th), trabecular number (Tb.N.), and trabecular separation (Tb.Sp). All measurements were performed in the CT imaging software CT-Analyzer (SkyScan 1174) in regions of interest (Figure S2, see Supplementary data) and with calibrations for bone mineral density. Micro-CT images were not available in 5 cases.
Histology
The cylindrical biopsies were cut perpendicular to the fracture line (see Figure 2) and embedded in paraffin after decalcification. 2 cases in the BP group were embedded undecalcified in poly(methyl methacrylate). Hematoxylin and eosin staining was performed for basic histologic assessment.
Bone histomorphometry and measurements of the fracture gap were performed by GZ, AL, and AF using the Olympus BX51 microscope (https://evidentscientific.com/en/search?q=Olympus+BX51+microscope+), the OsteoMeasure bone histomorphometry system (https://www.osteometrics.com/), and the cellSens Entry software (https://evidentscientific.com/en/products/software/cellsens). Using 10× magnification, an area of 100×60 μm was analyzed. The field-of-view was centered on the fracture gap and moved 60 μm (1 box) above or below the fracture gap using the tracing tool on each side of the initial box placement. The fracture gap width was measured at 5 equidistant points along the fracture line using the arbitrary line tool.
The number of osteocytes in a 750×250 μm section was counted using the 40× magnification objective. After centering on the fracture gap, the 750×250 μm grid was placed 250 μm above or below the fracture gap. Osteocyte lacunae were histologically categorized as alive if the osteocytes were present in osteocyte lacunae or were considered to be dead if the lacunae were empty. Giant osteoclasts were specifically sought [17]. GZ and AL individually assessed all the samples for the presence of loose bone fragments, woven bone close to the fracture line, cartilage adjacent to the fracture line, and osteoclasts and giant osteoclasts. These assessments were performed with the observers blinded to any background information, and consensus was reached.
Follow-up
All patients were followed up based on individual clinical assessments. All the available medical charts and radiographs obtained during clinical fracture care were reviewed to evaluate the postoperative course of healing, including reoperations and cortical bone healing at the biopsy site.
Statistics
The overall data were analyzed with descriptive statistics for frequencies, as percentages for categorical variables, and as means and standard deviations (SD) for continuous variables. Statistical analyses were performed using the IBM SPSS Statistics ver. 28 software (IBM Corp, Armonk, NY, USA). Methods to compensate for multiple comparisons were not applied.
Ethics, data sharing plan, funding, use of AI, and disclosures
The study was approved by the Ethical Review Board (Dnr. M14-09, 09-03-18 and Dnr. 2011/358-31, 11-11-23), and all patients had to provide oral and written consent before study inclusion. The study was funded by ALF grants Region Ostergötland (JS), Sweden, through generous support by the Knut and Alice Wallenberg Foundation and a post-doc research grant from the Centre of Research and Development, Region Gävleborg, Sweden. AI tools were not used. The authors report no conflicts of interest. Complete disclosure of interest forms according to ICMJE are available on the article page, doi: 10.2340/17453674.2025.43899
Results
Patients and background characteristics
19 patients fulfilled the following inclusion criteria: 50 years or older with a need for surgical treatment for incomplete AFF (Figure 1). All of the patients underwent surgical fixation due to thigh pain that persisted for > 4 weeks and impending fracture. There were 9 patients (5 women) with no BP use (non-BP group; mean age, 70 [SD 12] years; and 10 patients (9 women) with BP use for osteoporosis (BP group; mean age 77 [SD 11] years), with a mean duration of treatment of 6.7 years (SD 5.1). The median clinical follow-up was 9 months (range 2–20) in the non-BP group and 11.5 months (range 1–57) in the BP group. The median radiographic follow-up was 15 months (range 4–31) in the non-BP group and 12 months (range 2–57) in the BP group.
In the non-BP group, 3 patients had bone metabolic conditions. One patient had a clinical diagnosis of adynamic bone disease related to long-term chronic kidney disease and hemodialysis [18]. 1 patient had a diagnosis of X-linked hypophosphatemia, and 1 patient had a clinical suspicion of Paget’s disease of bone, treated with a single dose (5 mg) of zoledronic acid, 25 months before the AFF following the detection of a stress fracture lesion and signs of Paget’s disease on radiographs. As the stress fracture was already evident on MRI before the administration of zoledronic acid, this patient was assigned to the non-BP group. 2 patients had pathological structural variations of the femur geometry, 1 with coxa vara and 1 with extensive lateral bowing. Another patient suffered increasing pain after a period of intense manual labor (fatigue-type mechanism). In the remaining 3 patients, we found no clear causative factor for the AFF (Figure 5).
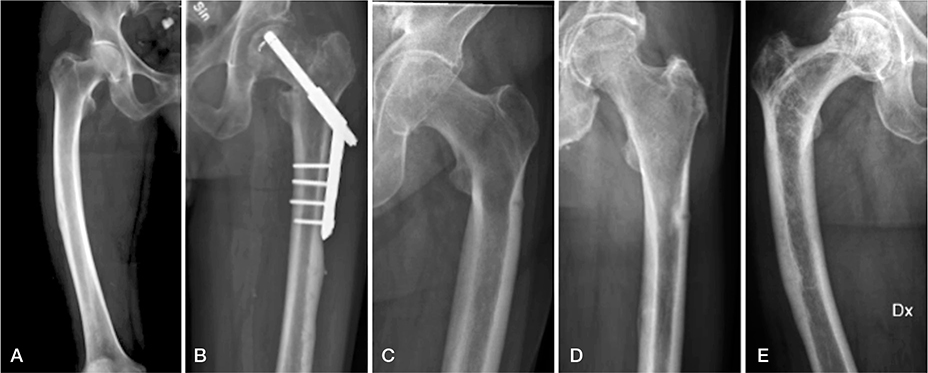
Figure 5. Potential pathologic mechanism in the non-BP group. A. Case 1, extensive lateral femoral bowing (CT-scout image). B. Case 3, adynamic bone disease. Note that the incomplete fractures are located below the plate fixation for the intertrochanteric fracture. C. Case 2, coxa vara. D. Case 8, hypophosphatemia. E. Case 9, Paget’s disease of bone. BP = bisphosphonate.
In the BP group, we noted some endocrinologic conditions that might affect bone health, albeit without strong associations to stress fractures (Table S2, see Supplementary data). 2 patients exhibited coxa vara and extensive lateral/anterior bowing.
Radiography
Fracture characteristics
All the plain radiographs showed lesions in the lateral cortex with surrounding focal cortical thickening, representing fracture callus (see Figure 3). In 6 patients in the non-BP group, the lesions were surrounded by an area of bone resorption and in 3 patients cortical irregularities could be seen (see Figure 4). In the BP group the fracture line was restricted to a well-defined line in all the patients (see Figure 3).
Fractures located in the mid-shaft region were observed in 9 patients in the BP group and 6 patients in the non-BP group. Multiple cortical lesions were observed in 2 patients in the BP group and 4 patients in the non-BP group (see Figure 4). Bilateral AFF were found in 3 patients in the BP group and 2 patients in the non-BP group.
Fracture healing
Radiologic signs of healing at the biopsy site (Figure S1, see Supplementary data) were observed within 1–4 months in all the patients in the non-BP group (Table S3, see Supplementary data) and in all but 1 patient in the BP group (Table 3 and Table S4, see Supplementary data).
3 patients had a complicated postoperative course despite successful fracture healing. In the non-BP group, 1 patient suffered a displaced refracture at the original fracture site 4.5 years after the index surgery (Figure S1, see Supplementary data). Another patient in the non-BP group, the patient with Paget’s disease of bone, suffered avascular necrosis of the femoral head. In the BP group, 1 patient suffered a new ipsilateral complete AFF proximal to the initial fracture, 5.7 years after the index surgery (Figure S3 and Table S4, see Supplementary data).
Micro-CT
The mean BV/TV was 18% lower in the non-BP group than in the BP group (47% vs 65%; 95% confidence interval [CI] –35 to –1.2). All other parameters were similar between the groups (Table S5 and Figure S4, see Supplementary data).
Histology and histomorphometry
The histologic findings confirmed those obtained in the micro-CT assessment. The mean BV/TV was 9.3% lower in the non-BP group than in the BP group (72% vs 81%; CI –16 to –2.9). All other parameters showed similar findings in both groups (Table 3 and Tables S6 and S7, see Supplementary data). Giant osteoclasts were observed only in the BP group (n = 7) (Figure S5, see Supplementary data) [19].
Discussion
We aimed to investigate the differences between AFF patients with and without BP treatment through studying the patients’ data from medical charts, radiographs, and bone biopsies from the fracture site. We found that 6 of the AFF patients in the non-BP group had some kind of bone pathology, whereas in the BP group there were no patients with metabolic bone disorders. Similar to other studies, the patients in the non-BP group were younger and more frequently male [4,20].
Radiography
In the assessment of plain radiographs, we found incomplete fractures in the non-BP group showing focal bone resorption around the fracture line instead of the well-defined dreaded black line in the BP group [13]. This pattern is similar to the stress lesions seen in the mid-shaft of the tibia of athletes, and is in line with current theories concerning the role of adaptive bone remodeling in the etiology of stress fractures [21,22]. Increased osteoclastic activity around the stress fracture lesion might also account for this phenomenon in the patients with AFF in the non-BP group, and it might also explain the lower BV/TV seen in the histologic analysis. These differences in radiologic fracture appearance, which have not been described previously, might impact future revisions of the ASBMR major criteria.
Extensive femoral bowing in combination with coxa vara was shown in the BP group, both of which are well-described risk factors for AFF [23]. We noted multiple cortical stress lesions in both groups [24]. This finding is rarely described in the literature, and its association with bone metabolic disease or deviating femoral geometry remains unclear.
Micro-CT and histology
Despite differences in the pathologic mechanisms, the histologic appearance at the fracture site and the bone in close vicinity to the fracture appeared to be similar in our 2 groups, except for the findings on plain radiographs described earlier. The only finding in the histologic analysis, confirmed by similar findings from the micro-CT analysis, was an increased bone tissue volume in relation to all tissue volume (BV/TV) in the BP group. This is likely an effect of BP, as the higher mean age in the BP group would result in lower bone tissue volumes, as compared with the younger patients in the non-BP group. Another possible explanation is that the lower bone tissue volume in the non-BP group is a result of increased remodeling as part of the healing of the stress fracture lesion, as described earlier [21]. However, we found no difference in the width of the fracture gap between the groups, which means that the increased remodeling was confined to the bone around the fracture rather than at the fracture surfaces themselves.
The giant osteoclasts, which are pathognomonic for BP treatment, were seen only in patients from the BP group [19]. In a study based on 2 patients with AFF (1 with BP and 1 without BP) from Japan, the authors noted hypertrophic osteoclasts, decreased bone resorption surface, decreased osteoclast numbers on the bone resorption surface, and an increased ratio of multinuclear osteoclasts, as well as misshapen and thin osteons and a higher mass and ratio of woven bone to total bone mass in the BP-treated patient [25]. Possible explanations for the non-significant findings regarding bone microstructure in our study include a small sample size and an associated risk of a Type II error. In addition, our bone samples were only representative of the bone tissue in close vicinity to the stress fracture lesion, where the fracture healing process might occlude the effect of the BP on the bone tissue. The inhomogeneous etiology in the non-BP group might cause dispersion of our findings, thereby smoothing the differences between the groups.
Limitations
The small sample size prohibits the making of any deductions based on statistically significant differences. Furthermore, we were restricted to the most basic investigations of bone microstructure available to us, which prohibited the analysis of BP-specific changes, such as microcracks [26]. We included only patients with symptomatic AFF necessitating prophylactic surgical fixation in both groups, which may have resulted in selection bias towards more severe cases. We also chose to include patients with underlying bone metabolic disease. However, no patients with these conditions were identified in the BP group. We believe that this approach yields a more representative sample of AFF patients in the clinical setting, where monogenic bone disorders, when looked for, appear to be relatively common [2,3].
Conclusion
We found small clinical differences between the BP and non-BP group related to bone metabolic diseases, deviations in whole bone geometry, and the radiologic appearance at the fracture site.
In perspective, a femoral stress fracture in the BP-naive patient should alarm the clinician to search for possible explanations including but not limited to bone metabolic diseases or deviations in whole-bone geometry.
Supplementary data
Supplementary Figures (S1–S5) and Supplementary Tables (S1–S7) are available in separate files on the article page, doi: 10.2340/17453674.2025.43899
- Ural A. Biomechanical mechanisms of atypical femoral fracture. J Mech Behav Biomed Mater 2021; 124: 104803. doi: 10.1016/j.jmbbm.2021.104803.
- Zhou W, van Rooij J G, van de Laarschot D M, Zervou Z, Bruggenwirth H, Appelman-Dijkstra N M, et al. Prevalence of monogenic bone disorders in a Dutch cohort of atypical femur fracture patients. J Bone Miner Res 2023. doi: 10.1002/jbmr.4801.
- Charoenngam N, Thongpiya J, Yingchoncharoen P, Ponvilawan B, Marangoz M S, Chenbhanich J, et al. Atypical femoral fracture in hypophosphatasia: a systematic review. Int J Endocrinol 2023; 2023: 5544148. doi: 10.1155/2023/5544148.
- Gani L U, Anthony N F, Dacay L M, Tan P T, Chong L R, King T F J. Characteristics of bisphosphonate and non-bisphosphonate related atypical femoral fracture in a South East Asian population: secondary analysis. Bone 2022; 162: 116455. doi: 10.1016/j.bone.2022.116455.
- Schilcher J, Michaelsson K, Aspenberg P. Bisphosphonate use and atypical fractures of the femoral shaft. N Engl J Med 2011; 364(18): 1728-37. doi: 10.1056/NEJMoa1010650.
- Bennell K L, Malcolm S A, Wark J D, Brukner P D. Models for the pathogenesis of stress fractures in athletes. Br J Sports Med 1996; 30(3): 200-4. doi: 10.1136/bjsm.30.3.200.
- Pentecost R L, Murray R A, Brindley H H. Fatigue, insufficiency, and pathologic frac-tures. JAMA 1964; 187(13): 1001-4. doi: 10.1001/jama.1964.03060260029006.
- Oh Y, Yamamoto K, Hashimoto J, Fujita K, Yoshii T, Fukushima K, et al. Biological activity is not suppressed in mid-shaft stress fracture of the bowed femoral shaft unlike in “typical” atypical subtrochanteric femoral fracture: a proposed theory of atypical femoral fracture subtypes. Bone 2020; 137: 115453. doi: 10.1016/j.bone.2020.115453.
- Black D M, Geiger E J, Eastell R, Vittinghoff E, Li B H, Ryan D S, et al. Atypical femur fracture risk versus fragility fracture prevention with bisphosphonates. N Engl J Med 2020; 383(8): 743-53. doi: 10.1056/NEJMoa1916525.
- Odvina C V, Zerwekh J E, Rao D S, Maalouf N, Gottschalk F A, Pak C Y. Severely suppressed bone turnover: a potential complication of alendronate therapy. J Clin Endocrinol Metab 2005; 90(3): 1294-301. doi: 10.1210/jc.2004-0952.
- Loi F, Cordova L A, Pajarinen J, Lin T H, Yao Z, Goodman S B. Inflammation, frac-ture and bone repair. Bone 2016; 86: 119-30. doi: 10.1016/j.bone.2016.02.020.
- Shane E, Burr D, Abrahamsen B, Adler R A, Brown T D, Cheung A M, et al. Atypical subtrochanteric and diaphyseal femoral fractures: second report of a task force of the American Society for Bone and Mineral Research. J Bone Miner Res 2014; 29(1): 1-23. doi: 10.1002/jbmr.1998.
- Koh J S, Goh S K, Png M A, Kwek E B, Howe T S. Femoral cortical stress lesions in long-term bisphosphonate therapy: a herald of impending fracture? J Orthop Trauma 2010; 24(2): 75-81. doi: 10.1097/BOT.0b013e3181b6499b.
- Mahjoub Z, Jean S, Leclerc J T, Brown J P, Boulet D, Pelet S, et al. Incidence and char-acteristics of atypical femoral fractures: clinical and geometrical data. J Bone Miner Res 2016; 31(4): 767-76. doi: 10.1002/jbmr.2748.
- Yoo H, Cho Y, Park Y, Ha S. Lateral femoral bowing and the location of atypical femo-ral fractures. Hip Pelvis 2017; 29(2): 127-32. doi: 10.5371/hp.2017.29.2.127.
- Lee K J, Kim B S, Kim K T, Jung G H. Three-dimensional morphologic features of Asian atypical femur and clinical implications of cephalomedullary nail fixation: computational measurement at actual size. Injury 2022; 53(12): 4090-8. doi: 10.1016/j.injury.2022.09.044.
- Schilcher J, Sandberg O, Isaksson H, Aspenberg P. Histology of 8 atypical femoral fractures: remodeling but no healing. Acta Orthop 2014; 85(3): 280-6. doi: 10.3109/17453674.2014.916488.
- Massy Z, Drueke T. Adynamic bone disease is a predominant bone pattern in early stages of chronic kidney disease. J Nephrol 2017; 30(5): 629-34. doi: 10.1007/s40620-017-0397-7.
- Weinstein R S, Roberson P K, Manolagas S C. Giant osteoclast formation and long-term oral bisphosphonate therapy. N Engl J Med 2009; 360(1): 53-62. doi: 10.1056/NEJMoa0802633.
- Schilcher J, Koeppen V, Aspenberg P, Michaelsson K. Risk of atypical femoral fracture during and after bisphosphonate use. Acta Orthop 2015; 86(1): 100-7. doi: 10.3109/17453674.2015.1004149.
- Schilcher J, Bernhardsson M, Aspenberg P. Chronic anterior tibial stress fractures in athletes: no crack but intense remodeling. Scand J Med Sci Sports 2019; 29(10): 1521-8. doi: 10.1111/sms.13466.
- Hughes J M, Popp K L, Yanovich R, Bouxsein M L, Matheny R W Jr. The role of adaptive bone formation in the etiology of stress fracture. Exp Biol Med (Maywood) 2017; 242(9): 897-906. doi: 10.1177/1535370216661646.
- Starr J, Tay Y K D, Shane E. Current understanding of epidemiology, pathophysiology, and management of atypical femur fractures. Curr Osteoporos Rep 2018; 16(4): 519-29. doi: 10.1007/s11914-018-0464-6.
- Png M A, Mohan P C, Koh J S B, Howe C Y, Howe T S. Natural history of incom-plete atypical femoral fractures in patients after a prolonged and variable course of bisphospho-nate therapy: a long-term radiological follow-up. Osteoporos Int 2019; 30(12): 2417-28. doi: 10.1007/s00198-019-05067-7.
- Aki T, Hashimoto K, Uozumi H, Saito M, Sugawara K, Suzuki M, et al. Morphological and morphometrical analyses of fracture-healing sites of an atypical femoral fracture in patients with and without long-term bisphosphonate treatment for osteoporosis: a report of two cases. Tohoku J Exp Med 2021; 253(4): 261-7. doi: 10.1620/tjem.253.261.
- Somford M P, van Ruijven L J, Kloen P, Bakker A D. Histological and micro computed tomography analysis of a femoral stress fracture associated with prolonged bisphosphonate use. Clin Cases Miner Bone Metab 2017; 14(1): 92-6. doi: 10.11138/ccmbm/2017.14.1.092.
- Nguyen H H, van de Laarschot D M, Verkerk A, Milat F, Zillikens M C, Ebeling P R. Genetic risk factors for atypical femoral fractures (AFFs): a systematic review. JBMR Plus 2018; 2(1): 1-11. doi: 10.1002/jbm4.10024.
- Franceschetti P, Bondanelli M, Caruso G, Ambrosio M R, Lorusso V, Zatelli M C, et al. Risk factors for development of atypical femoral fractures in patients on long-term oral bisphosphonate therapy. Bone 2013; 56(2): 426-31. doi: 10.1016/j.bone.2013.07.010.
- Clegg S M, Eiel E S, Fine S, Gafni R I, Most M J. Atypical fragility fractures due to bony or soft tissue phosphaturic mesenchymal tumors: a report of two cases. Case Rep Orthop 2023; 2023: 5614065. doi: 10.1155/2023/5614065.
- Girgis C M, Sher D, Seibel M J. Atypical femoral fractures and bisphosphonate use. N Engl J Med 2010; 362(19): 1848-9. doi: 10.1056/NEJMc0910389.
- Lee I, Son D-W, Park J H, Park J H. Drug-induced hyperprolactinemia results in atypi-cal atypical fracture. Hip Pelvis 2021; 33(2): 102-7. doi: 10.5371/hp.2021.33.2.102.
- Berger G K, Graf A R, Wooldridge A N, Hackbarth D A. Complex femoral reconstruc-tion following pathologic subtrochanteric femur fracture secondary to Paget’s disease of the bone: a case report with long-term follow-up. J Orthop Case Rep 2020; 10(3): 19-22. doi: 10.13107/jocr.2020.v10.i03.1730.
- Popp K L, Caksa S, Martinez-Betancourt A, Yuan A, Tsai J, Yu E W, et al. Cortical bone material strength index and bone microarchitecture in postmenopausal women with atypi-cal femoral fractures. J Bone Miner Res 2019; 34(1): 75-82. doi: 10.1002/jbmr.3590.
- Farr J N, Drake M T, Amin S, Melton L J 3rd, McCready L K, Khosla S. In vivo as-sessment of bone quality in postmenopausal women with type 2 diabetes. J Bone Miner Res 2014; 29(4): 787-95. doi: 10.1002/jbmr.2106.
- Lim S J, Yeo I, Yoon P W, Yoo J J, Rhyu K H, Han S B, et al. Incidence, risk factors, and fracture healing of atypical femoral fractures: a multicenter case-control study. Osteoporos Int 2018; 29(11): 2427-35. doi: 10.1007/s00198-018-4640-4.
- Koh J H, Myong J P, Jung S M, Lee J, Kwok S K, Park S H, et al. Atypical femoral fracture in rheumatoid arthritis patients treated with bisphosphonates: a nested case-control study. Arthritis Rheumatol 2016; 68(1): 77-82. doi: 10.1002/art.39429.
Appendix
| Disease | Number of patients/fracture significance | Suggested mechanism | References |
| Hypophosphatemia | 4 | Hypophosphatasia is a metabolic disorder marked by low levels of alkaline phosphatase (ALP). In adults, skeletal manifestations may present as osteopenia, poorly healing stress fractures in the metatarsal bones, and pseudo-fractures that are typically found on the lateral side of the femoral shaft, which can resemble BP-associated AFFs | Nguyen et al. 2018 [27] |
| Pycnodysostosis | 7 | Impairment of osteoclast function results in osteosclerosis, abnormal bone matrix, increased bone density, and brittleness, increasing the risk of pathologic fractures in the long bones | – |
| Osteopetrosis | 4 | Failure of osteoclast-mediated bone resorption leads to increased bone mass. Although the bone density is increased, the sclerotic bone is brittle, leading to fragility fractures | – |
| Osteoporosispseudoglioma syndrome | 1 | Autosomal recessive type of juvenile osteoporosis. Loss-of-function mutation in the LRP5 gene, which regulates bone formation, leads to primary osteoblast dysfunction | – |
| Osteogenesis imperfecta | 5 | A connective tissue disorder characterized by distinct skeletal features, such as reduced bone mass, hypermineralized bone matrix, numerous fragility fractures, bone deformities, and short stature | – |
| X-linked osteoporosis | 1 | Pathogenic variants in the PLS3 gene, located on the X chromosome, have been linked to skeletal fragility in hemizygous males, whereas heterozygous females may exhibit a range of clinical phenotypes, from normal bone mineral density with no fractures to early-onset osteoporosis | – |
| X-linked hypophosphatemia | 1 | Common characteristics of this condition include low bone mineral density, rickets and/or osteomalacia, along with shortening and deformities of the lower limbs, which increase the susceptibility to fractures | – |
| Hypocalcemia/subclinical hypoparathyroidism | 11 AFF vs 58 normal femur fractures (odds ratio 15, CI 2.9–80) | Extended periods of hypocalcemia can lead to inadequate bone formation and brittle bones that are more susceptible to fractures. As PTH stimulates bone turnover, reduced PTH levels may worsen the already suppressed bone remodeling seen in patients treated with BPs | Franceschetti et al. 2013 [28] |
| Tumor-induced osteomalacia | 2 | A rare paraneoplastic disorder. Typically, benign phos-phaturic mesenchymal tumors secrete excessive amounts of fibroblast growth factor-23 (FGF23), resulting in hypophosphatemia, muscle weakness, and an increased risk of fractures | Clegg et al. 2023 [29] |
| Vitamin D deficiency | 20 AFF vs 152 normal femur fractures (odds ratio 3.5, CI 1.7–19) | Vitamin D deficiency-induced secondary osteomalacia may increase the risks for stress and fragility fractures | Girgis et al. 2010 [30] |
| Hyperprolactinemia | 1 | Hyperprolactinemia (in this case associated with antipsychotic medication use) suppresses the release of GnRH from the hypothalamus, which in turn causes hypogonadism that contributes to bone loss. Recent research has uncovered additional hormonal factors that may disrupt bone homeostasis, such as reduced calcitonin plasma levels in hyperprolactinemic women, or elevated parathyroid hormone-related peptide levels in the plasma of women with prolactinoma | Lee et al. 2021 [31] |
| Paget’s disease of bone | 1 | This condition is marked by an imbalance in the process of bone resorption and formation. It is thought that a defect in osteoclast function causes disorganized bone resorption resulting in inadequate bone formation, bones that are biomechanically weaker, structurally disorganized, less dense, hypervascularized, and more susceptible to fractures and deformation under stress | Berger et al. 2020 [32] |
| Diabetes | 15 AFF vs 20 normal femur fractures. 20% (n = 3) vs. 10% (n = 2) P < 0.05 | Similar to the effects of high-dose bisphosphonate treatment, extended periods of low bone turnover in type 2 diabetes can lead to elevated levels of advanced glycation end-products in bone, impairment of microdamage repair, and accumulation of bone microcracks, increasing the risk of fractures | Popp et al. 2019 [33] Joshua et al. 2014 [34] |
| Rheumatoid arthritis | 196 AFF vs 94 normal femur fractures (crude odds ratio 11, CI 1.4–80) P = 0.02 | Patients with rheumatoid arthritis generally exhibit reduced bone mineral density compared with healthy individuals. Factors that contribute to increased bone loss include age, degree of disability, low body mass index, prolonged duration of the disease, systemic inflammation associated with the condition, and extended use of gluco-corticoids | Lim et al. 2018 [35] Koh et al. 2016 [36] |