How good are surgeons at disclosing periprosthetic joint infection at the time of revision, based on pre- and intra-operative assessment? A study on 16,922 primary total hip arthroplasties reported to the Norwegian Arthroplasty Register
Olav LUTRO 1, Synnøve MO 2, Marianne Bollestad TJØRHOM 1, Anne Marie FENSTAD 2, Tesfaye Hordofa LETA 2,6, Trond BRUUN 3, Geir HALLAN 2,3, Ove FURNES 2,5, and Håvard DALE 2,5
1 Department of Medicine, Stavanger University Hospital, Stavanger; 2 The Norwegian Arthroplasty Register, Department of Orthopaedic Surgery, Haukeland University Hospital, Bergen; 3 Department of Medicine, Haukeland University Hospital, Bergen; 4 Department of Clinical Science, University of Bergen, Bergen; 5 Department of Clinical Medicine, University of Bergen, Bergen; 6 VID Specialized University, Bergen, Norway
Background and purpose — Revision due to infection, as reported to the Norwegian Arthroplasty Register (NAR), is a surrogate endpoint to periprosthetic joint infection (PJI). We aimed to find the accuracy of the reported causes of revision after primary total hip arthroplasty (THA) compared with PJI to see how good surgeons were at disclosing infection, based on pre- and intraoperative assessment.
Patients and methods — We investigated the reasons for revision potentially caused by PJI following primary THA: infection, aseptic loosening, prolonged wound drainage, and pain only, reported to the NAR from surgeons in the region of Western Norway during the period 2010–2020. The electronic patient charts were investigated for information on clinical assessment, treatment, biochemistry, and microbiological findings. PJI was defined in accordance with the Musculoskeletal Infection Society (MSIS) definition. Sensitivity, specificity, and accuracy were calculated.
Results — 363 revisions in the NAR were eligible for analyses. Causes of revision were (reported/validated): infection (153/177), aseptic loosening (139/133), prolonged wound drainage (37/13), and pain only (34/40). The sensitivity for reported revision due to infection compared with PJI was 80%, specificity was 94%, and accuracy—the surgeons’ ability to disclose PJI or non-septic revision at time of revision—was 87%. The accuracy for the specific revision causes was highest for revision due to aseptic loosening (95%) and pain only (95%), and lowest for revision due to prolonged wound drainage (86%).
Conclusion — The accuracy of surgeon-reported revisions due to infection as representing PJI was 87% in the NAR. Our study shows the importance of systematic correction of the reported cause of revision in arthroplasty registers, after results from adequately taken bacterial samples.
Citation: Acta Orthopaedica 2024; 95: 67–72. DOI https://doi.org/10.2340/17453674.2024.39914.
Copyright: © 2024 The Author(s). This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (https://creativecommons.org/licenses/by-nc/4.0/), allowing third parties to copy and redistribute the material in any medium or format and to remix, transform, and build upon the material for non-commercial purposes, provided proper attribution to the original work.
Submitted: 2023-09-28. Accepted: 2023-12-14. Published: 2024-01-30.
Correspondence: olav.lutro@sus.no
HD and OF were the initiators of this study. SM, HD, and OL collected the data from the electronic health record system. OL performed the analyses of the data and wrote the manuscript. All authors contributed to the conception and design of the study, critical analyses of the data, interpretation of the findings, and critical revision of the manuscript through all stages of the study.
The authors thank all Norwegian surgeons for conscientiously reporting THAs to the NAR, and the secretaries, IT analyst, and statisticians at the NAR for entering the data and preparing them for analyses.
Handling co-editor: Bart A. Swierstra
Acta thanks Martin Clauss and Jon Goosen for help with peer review of this manuscript.
It is common practice to do bacterial sampling during implant revision of a THA. In some cases, results from these samples can alter the diagnosis as cause of the revision from aseptic to septic loosening when bacterial cultures confirm that the cause was periprosthetic joint infection (PJI). In such cases, the diagnosis of aseptic loosening would remain uncorrected and erroneous in the register. This has raised concerns that register studies on revisions due to infection after total hip arthroplasty (THA) are inaccurate and may misrepresent the true incidence of PJI [1].
2 of the most common causes of revision reported to the Norwegian Arthroplasty Register (NAR) are deep infection and aseptic loosening [2]. As implants and surgical techniques have improved over the last decades, fewer accounts of aseptic loosening have been reported and infection has emerged as one of the most common causes of revision in the NAR [2]. One has speculated whether this may partly be due to improved diagnostics and higher awareness and reporting of low-grade infections [3].
The primary aim of our study was to validate reporting of revision due to infection in the NAR, to determine how well surgeons disclosed PJI at the time of revision based on pre- and intraoperative assessment. The secondary aim was to investigate how often reported revisions due to aseptic loosening, prolonged wound drainage, and pain only were PJIs.
Patients and methods
Materials/setting
The study was conducted in accordance with the STARD statement.
The NAR has gathered data on THA, both primary and revision surgery, since 1987. The surgeon reports on a form (paper or electronically) immediately after surgery. The collected data includes information on the indication for surgery, like cause of a revision [4]. Studies have found 97% completeness of reporting of primary THAs, 91–94% reporting of revisions, and 100% reporting of deaths [2].
Western Norway Regional Health Authority is 1 of 4 health trusts in Norway. It is part of the public health services and is the administrative body of 12 public hospitals in Western Norway. The health trust hospitals cover approximately 20% of the Norwegian population. All hospitals use the same electronic health record system. This contains all clinical information including clinical assessments, surgery reports, as well as laboratory and microbiology results.
In the present study completeness of reporting was 97% for primary THA and 92% for first revisions in the study population, compared with 97% and 91% respectively in the rest of Norway, validated against the Norwegian Patient Register (Table 1).
In Norway, THA surgery is performed at local, university, and specialized orthopedic hospitals, all of which are represented in the study. The study population therefore is expected to be representative of the national population (high external validity).
Selection
The reported causes of revision considered to potentially represent PJI, anticipated or not, were infection, aseptic loosening, prolonged wound drainage (imminent infection through intra- or postoperative contamination), and pain only (potential low-grade infection).
Cases that were revised with the removal or exchange of implant parts, as well as soft tissue debridement without the exchange of hardware, were included.
We defined PJI in accordance with the major criteria in the Musculoskeletal Infection Society (MSIS) definition [5]. Hence, growth of phenotypically identical bacteria in 2 or more intraoperative bacterial cultures was considered proof of an infection, as was a chronic fistula communicating with the prosthesis. When growth in only 1 of at least 5 samples appeared, we assessed other information, such as CRP above 10 mg/L, presence of purulence, and type of bacteria. A single positive sample with high-virulence bacteria (Staphylococcus aureus, Streptococci spp., Enterococci spp., or gram-negative rods) confirmed a PJI whereas low-virulent bacteria in 1 sample would not. Use of histopathological samples was very limited, as was the use of other markers in synovial fluid. Bacterial findings in synovial fluid preoperatively were considered proof of infection only if supported by either blood culture findings or tissue samples of the same bacteria.
Intraoperative tissue sampling and handling in the microbiology laboratories are standardized nationally, with a recommendation of at least 5 samples being collected, and with an incubation time of at least 7 days [6,7].
Statistics
We calculated the sensitivity, specificity, and accuracy of reported data as presented in Table 2.
Sensitivity is the probability of the reported revision due to infection representing PJI (inclusion of true positives), hence the surgeons’ ability to disclose PJI when the patient is suspected to have PJI clinically. Specificity is the ability to exclude PJI, when the reported revision cause is suspected to be other than infection (exclusion of true negatives), hence the ability to exclude PJI. Accuracy is the surgeons’ ability to disclose either PJI or non-septic revision as the correct cause of the revision immediately after revision surgery of potential PJI cases. In other words, accuracy represents the surgeons’ ability to differentiate the infected and non-infected cases correctly at the time of surgery.
Ethics, data sharing plan, funding, and disclosures
The Regional Ethics Committee approved the study, REK 209074 (2021). The registration of data and the study was performed confidentially on patient consent and according to Norwegian and EU data protection rules. The study was fully financed by the NAR. No conflict of interest is declared. Data may be accessible upon application to NAR. Complete disclosure of interest forms according to ICMJE are available on the article page, doi: 10.2340/17453674.2024.39914
Results
16,922 primary THAs with 632 revisions due to any cause were reported to the NAR from the region in the period 2010–2020 (Figure). In addition, the non-included THA patients from the rest of Norway are presented in Table 1 for demonstration of representability. Table 1 shows the baseline demographic and clinical characteristics of the study cohort from Western Norway compared with the national primary THA cohort. The Figure shows the selection of revisions possibly due to PJI eligible for further analyses.
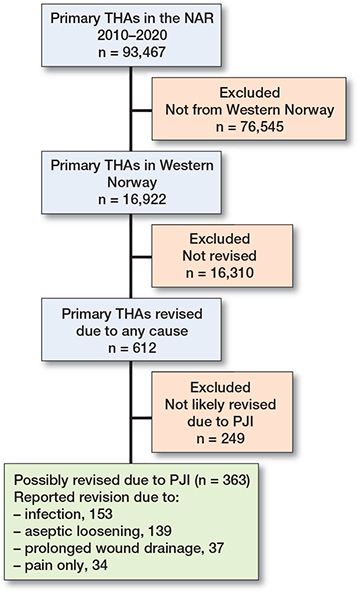
Flowchart of the selection of THAs eligible for inclusion, i.e., reported to NAR as revised in Western Norway Health Authority hospitals from 2010–2020 for the causes, infection, aseptic loosening, prolonged wound drainage, or pain only.
Among the 363 revisions reported and assessed, there were 153 reported revisions due to infection, 139 due to aseptic loosening, 37 due to prolonged wound drainage, and 34 due to pain only (Table 3).
After workup with examination of bacterial cultures and clinical data, 177 cases were classified as PJI, 133 as aseptic loosening, 13 as prolonged wound drainage (no infection), and 40 as pain only (Table 3).
Specificity, sensitivity, and accuracy are presented in Table 4. Only 141 of the 177 PJIs were reported by the surgeon to be caused by infection, which results in an overall sensitivity of 80% for reported revisions due to infection. The corresponding specificity was 94%. The probability that surgeons will correctly diagnose and report PJI or aseptic causes immediately after surgery (accuracy) was 87%.
The probability that the reported cause was correct and not actually caused by PJI (accuracy) was highest for aseptic loosening and pain only (both 95%), and lowest for prolonged wound drainage (86%).
Discussion
We aimed to validate reporting of revision due to infection in the NAR, to determine how well surgeons disclosed PJI at the time of revision based on pre- and intraoperative assessment. We found that the probability that surgeons correctly diagnosed and reported PJI immediately after revision surgery was 87%, resulting in a misdiagnosis of 13%. The sensitivity of reported revisions due to infection in NAR was 80%, whereas the specificity was 94%.
Revisions due to aseptic loosening or pain only reported to the NAR rarely represented PJI, whereas the majority of revisions due to prolonged wound drainage represented PJI.
At the time of bacterial sampling and reporting immediately after surgery, the results of bacteriological cultures are not available for the surgeon. The cause for revision will therefore be based on the presenting signs and symptoms in addition to preoperative assessment. To diagnose PJI or other causes of revision may be difficult, and will always involve some degree of uncertainty. This may lead to some degree of misdiagnosis when reporting to the NAR, as found in our study.
Infection vs. aseptic loosening
Low-grade infections can be difficult to distinguish from aseptic loosening. One of the main theories for aseptic loosening is that it is caused by an inflammatory reaction to wear particles from the articulation in a complex pathway leading to increased osteoclastic activity and loosening of the prosthesis [8]. A similar process can be seen in PJI, where low-grade infection in organized biofilms can produce an inflammatory response with a subsequent loosening of the prosthesis [8]. In these cases, histology may be helpful to distinguish between infection and inflammation, but this is not commonly used in Norway. A previous study from NAR found that systemic antibiotic prophylaxis reduced the risk of both aseptic and septic revisions [9]. This led to the speculation that some cases of assumed aseptic loosening were in fact deep infections.
The accuracy of the reported revisions due to aseptic loosening of 95% relative to PJI in our study is in accordance with other studies that present prevalence of unsuspected PJI between 3% and 12% [10-12].
The implications of missed infections could be the need for repeat major revisions, patient suffering, a poor clinical outcome, and increased cost [13]. Some studies, however, have shown limited damage in the case of missed infections in revisions due to suspected aseptic loosening [11,14].
Infection vs. prolonged wound drainage
In the present study, two-thirds of revisions due to prolonged wound drainage represented PJI based on results of intraoperative bacterial cultures.
The definition of prolonged wound drainage is not clearcut in the literature, nor is its management. In a review, the authors found that different studies have used duration from 2 to 7 days, and various degrees of quantification, for instance 2 x 2 cm of drainage in the wound dressing beyond 72 hours after index surgery [15].
A recent Dutch study showed strong association between wound drainage and PJI from the 2nd week after surgery [16].
Prolonged wound drainage has been shown to be an independent risk factor for the development of PJI, as it represents a pathway for bacteria to deeper tissues [16,17]. Therefore, prolonged wound drainage could represent imminent PJI, and it is recommended to approach it with surgical measures, including debridement, thorough lavage, and exchange of modular parts. During surgical debridement, adequate tissue samples should be taken for microbiological culturing [15]. The surgeon will normally treat with empiric antibiotics systemically until bacterial results are known, in accordance with guidelines. Hence, most reported revisions due to prolonged wound drainage in our study that represented PJI were due to the timing of reporting and did not reflect misdiagnosed PJI. In other words, the cause of the revision is reported correctly because it was not possible to disclose the PJI status at the time of reporting.
For this reason, one can argue that prolonged wound drainage is the correct diagnosis to report after an early revision due to unexpected long wound secretion after THA, even if performed due to the suspicion or risk of PJI.
Infection vs. pain only
In our study, 3 out of 34 revisions initially reported to be due to pain only turned out to be infected. The diagnosis of PJI can be challenging, and when pain is the only or the predominant symptom, low-grade infections may be overlooked [13,18].
Although there were few false negative revisions due to pain only in this study, it again highlights the importance of intraoperative tissue samples for bacterial culture in all surgical revisions where infection is impossible to rule out.
Strengths
Norway has a public healthcare system where hospital inpatient treatment is provided free of charge. We believe this results in a good level of follow-up on complications, as socioeconomic status will not affect the patients’ ability to receive treatment. The revision surgery is performed in public hospitals exclusively. In Norway, the use of antibiotics is under relatively strict stewardship directed by national guidelines and under routine surveillance [19,20]. There is a national Advisory Unit for Antibiotic Use in Hospitals, which, among other duties, systematically surveils national antibiotics stewardship programs [19]. Extensive use of empiric antibiotic treatment prior to revision surgery will result in negative intraoperative cultures, and more empiric than targeted antibiotic treatment when PJI is suspected. Therefore, surgeons strive to keep the patient off antibiotics for 14 days before taking samples when considered safe and PJI is suspected. This is expected to result in few culture-negative infections [21]. The handling of PJI is described in national guidelines, where both medical and surgical sampling, treatment, and the handling of samples in the microbiology laboratories are described [6,7].
All hospitals report to NAR, hence a revision performed at a hospital other than the primary one will be captured if reported and linked to the primary THA through a unique personal identification number. Hence, the capture rate for primary (98%) and revision (91%) THA is considered good for a national arthroplasty register (and our regional cohort), but not complete, since the NAR depends on conscientious reporting by Norwegian surgeons.
In the present study all the information needed regarding preoperative antibiotics, culture results, surgery reports, and lab results was available in a uniform electronic health record. We found high yield in the intraoperative bacterial cultures and followed the patients both regarding THA survival in NAR, and their clinical course in the electronic health record during the study period. This information, including clinical assessments and course, surgery reports, as well as laboratory and microbiological results, combined with revision causes, enabled us to get a near complete picture of the individual cases. We therefore expect the validation to be of high quality.
Limitations
The present study is only based on 1 of the 4 health trusts in Norway. However, we have reason to believe that clinical practice has limited variation throughout the country, which is why the results may have external validity in Norway. This is supported by the findings of similar demographics, risk factors, prevalence of revision causes, and time to revision between the study population and the rest of Norway [2].
We have examined the revisions reported to NAR. A Danish study to find the “true” incidence of PJI estimated 40% more PJI than reported to the Danish Hip Arthroplasty Register [22]. Hence, some PJIs not treated with revision surgery could be missed. However, we found completeness of reporting of any revisions at 91% in the present study. A prevalence of revision due to infection in NAR at 1.3 % has been shown in previous studies, which compares well to the “true incidence” of 1.0 % in the Danish study. Furthermore, there is an increase in the incidence of early revision through debridement and implant retention, and we believe that not many PJIs in the THA population will be treated without surgery. We do not have reason to believe that the completeness of reporting of revision due to infection is lower than for any revision [2,3,23].
When considering the revisions due to infection, we used the parameter of 2 or more periprosthetic samples with growth of phenotypically identical organisms. This is a major criterion in the MSIS and a confirmatory criterion in the EBJIS definition of PJI [5,13]. However, we did not systematically use minor criteria, such as CRP, ESR, elevated synovial white blood cell counts or leucocyte esterase, positive alpha defensin, histopathology, or sonication. Hence, we might to some extent have underestimated cases of culture negative PJI. In Norway, it is not common practice to use an alpha defensin test, and histopathology is undertaken rarely. Norwegian microbiology laboratories do not use sonication of explanted prostheses [7]. This may also result in some underestimation of actual PJI in the present study.
Reported causes of revision may have several biases. The reporting surgeon may be unaware of low-grade infections, with its subtle presentation, and therefore fails to diagnose PJI before and during surgery [13,18,24]. In other cases, the reporting surgeon may be subject to “wishful thinking” as infection may be a devastating outcome of otherwise successful surgery. Also, reporting a perceived less devastating cause of revision may maintain better surveillance statistics, as the reported cause is not to be corrected later, so-called “gaming” [25,26].
Conclusion
The accuracy of surgeon-reported revisions due to infection as actually representing PJI was 87% in the NAR, which overall is good. This study shows how good the surgeons are at disclosing PJI as the cause of THA revision at time of surgery.
Perspective
From 2023, NAR has introduced a validation form sent to the reporting surgeon 3 weeks after THA revisions due to infection, aseptic loosening, prolonged wound drainage, or pain alone, for systematic confirmation/correction of the reported revision cause after the results from bacterial samples.
This form is similar to the form used in the register-randomized controlled study on total knee arthroplasty (the ALBA study) [27], as well as in our study.
We believe this will improve the quality and accuracy of endpoint revision due to PJI, as well as non-infected endpoints, in future research.
- Witso E. The rate of prosthetic joint infection is underestimated in the arthroplasty registers. Acta Orthop 2015; 86: 277-8. doi: 10.3109/17453674.2015.1042320.
- Norwegian Arthroplasty Register—Annual Report 2022. Norwegian Arthroplasty Register; 2022. Available from: https://helse-bergen.no/seksjon/Nasjonal_kompetansetjeneste_leddproteser_hoftebrudd/Share%20point%20Documents/Rapport/Report%202022%20english.pdf.
- Dale H, Hovding P, Tveit S M, Graff J B, Lutro O, Schrama J C, et al. Increasing but levelling out risk of revision due to infection after total hip arthroplasty: a study on 108,854 primary THAs in the Norwegian Arthroplasty Register from 2005 to 2019. Acta Orthop 2021; 92: 208-14. doi: 10.1080/17453674.2020.1851533.
- Havelin L I, Engesaeter L B, Espehaug B, Furnes O, Lie S A, Vollset S E. The Norwegian Arthroplasty Register: 11 years and 73,000 arthroplasties. Acta Orthop Scand 2000; 71: 337-53. doi: 10.1080/000164700317393321.
- Parvizi J, Tan T L, Goswami K, Higuera C, Della Valle C, Chen A F, et al. The 2018 definition of periprosthetic hip and knee infection: an evidence-based and validated criteria. J Arthroplasty 2018; 33: 1309-1314.e1302. doi: 10.1016/j.arth.2018.02.078.
- Helsedirektoratet. Müller-Indrebø E, editor. Guideline for treating prosthetic joint infections in Norwegian hospitals [in Norwegian]; 2022. Available from: https://www.helsedirektoratet.no/retningslinjer/antibiotika-i-sykehus/ben-og-leddinfeksjoner/proteseinfeksjon-protesebevarende-eller-en-seanse-kirurgi#proteseinfeksjon-protesebevarende-elleren-seanse-kirurgi-empirisk-praktisk.
- Wik Larssen K. Microbiological diagnostics in orthopedic infections [in Norwegian]; online 2023 [cited 17.03.2023]. Available from https://www.fhi.no/contentassets/f47318f177dd4c83b87ecd7a0a0701ce/strategirapport-ortopediske-infeksjoner.pdf
- Hodges N A, Sussman E M, Stegemann J P. Aseptic and septic prosthetic joint loosening: impact of biomaterial wear on immune cell function, inflammation, and infection. Biomaterials 2021; 278: 121127. doi: 10.1016/j.biomaterials.2021.121127.
- Engesaeter L B, Lie S A, Espehaug B, Furnes O, Vollset S E, Havelin L I. Antibiotic prophylaxis in total hip arthroplasty: effects of antibiotic prophylaxis systemically and in bone cement on the revision rate of 22,170 primary hip replacements followed 0–14 years in the Norwegian Arthroplasty Register. Acta Orthop Scand 2003; 74: 644-51. doi: 10.1080/00016470310018135.
- Renard G, Laffosse J M, Tibbo M, Lucena T, Cavaignac E, Rouvillain J L, et al. Periprosthetic joint infection in aseptic total hip arthroplasty revision. Int Orthop 2020; 44: 735-41. doi: 10.1007/s00264-019-04366-2.
- Hipfl C, Mooij W, Perka C, Hardt S, Wassilew G I. Unexpected lowgrade infections in revision hip arthroplasty for aseptic loosening: a single-institution experience of 274 hips. Bone Joint J 2021; 103-b: 1070-77. doi: 10.1302/0301-620x.103b6.Bjj-2020-2002.R1.
- Fernandez-Sampedro M, Salas-Venero C, Fariñas-Álvarez C, Sumillera M, Pérez-Carro L, Fakkas-Fernandez M, et al. Postoperative diagnosis and outcome in patients with revision arthroplasty for aseptic loosening. BMC Infect Dis 2015; 15: 232. doi: 10.1186/s12879-015-0976-y.
- McNally M, Sousa R, Wouthuyzen-Bakker M, Chen A F, Soriano A, Vogely H C, et al. The EBJIS definition of periprosthetic joint infection. Bone Joint J 2021; 103-b: 18-25. doi: 10.1302/0301-620x.103b1.Bjj-2020-1381.R1.
- Boot W, Moojen D J, Visser E, Lehr A M, De Windt T S, Van Hellemondt G, et al. Missed low-grade infection in suspected aseptic loosening has no consequences for the survival of total hip arthroplasty. Acta Orthop 2015; 86: 678-83. doi: 10.3109/17453674.2015.1086942.
- Wagenaar F B M, Löwik C A M, Zahar A, Jutte P C, Gehrke T, Parvizi J. Persistent wound drainage after total joint arthroplasty: a narrative review. J Arthroplasty 2019; 34: 175-82. doi: 10.1016/j.arth.2018.08.034.
- Scheper H, Mahdad R, Elzer B, Löwik C, Zijlstra W, Gosens T, et al. Wound drainage after arthroplasty and prediction of acute prosthetic joint infection: prospective data from a multicentre cohort study using a telemonitoring app. J Bone Joint Infect 2023; 8: 59-70. doi: 10.5194/jbji-8-59-2023.
- Zhu Y, Zhang F, Chen W, Liu S, Zhang Q, Zhang Y. Risk factors for periprosthetic joint infection after total joint arthroplasty: a systematic review and meta-analysis. J Hosp Infect 2015; 89: 82-9. doi: 10.1016/j.jhin.2014.10.008.
- Rienmüller A, Borens O. Propionibacterium prosthetic joint infection: experience from a retrospective database analysis. Eur J Orthop Surg Traumatol 2016; 26: 429-34. doi: 10.1007/s00590-016-1766-y.
- Skodvin B, Høgli J U, Gravningen K, Neteland M I, Harthug S, Akselsen P E. Nationwide audit and feedback on implementation of antibiotic stewardship programmes in Norwegian hospitals. JAC Antimicrob Resist 2021; 3: dlab063. doi: 10.1093/jacamr/dlab063.
- Helsedirektoratet. National Health Care Quality Indicators [in Norwegian]; online 2023 [cited 2023]. Available from https://www.helse-direktoratet.no/statistikk/kvalitetsindikatorer/legemidler/forbruk-av-etutvalg-bredspektrede-antibiotika-i-norske-sykehus
- Trampuz A, Piper K E, Jacobson M J, Hanssen A D, Unni K K, Osmon D R, et al. Sonication of removed hip and knee prostheses for diagnosis of infection. N Engl J Med 2007; 357: 654-63. doi: 10.1056/NEJMoa061588.
- Gundtoft P H, Overgaard S, Schønheyder H C, Møller J K, Kjærsgaard-Andersen P, Pedersen A B. The “true” incidence of surgically treated deep prosthetic joint infection after 32,896 primary total hip arthroplasties: a prospective cohort study. Acta Orthop 2015; 86: 326-34. doi: 10.3109/17453674.2015.1011983.
- Dale H, Fenstad A M, Hallan G, Overgaard S, Pedersen A B, Hailer N P, et al. Increasing risk of revision due to infection after primary total hip arthroplasty: results from the Nordic Arthroplasty Register Association. Acta Orthop 2023; 94: 307-15. doi: 10.2340/17453674.2023.13648.
- Pérez-Prieto D, Hinarejos P, Alier A, Sorlí L, Martínez S, Puig L, et al. Adherence to a reliable PJI diagnostic protocol minimizes unsuspected positive cultures rate. BMC Musculoskelet Disord 2021; 22: 653. doi: 10.1186/s12891-021-04431-1.
- Antonacci A C, Dechario S P, Antonacci C, Husk G, Patel V, Nicastro J, et al. Cognitive bias impact on management of postoperative complications, medical error, and standard of care. J Surg Res 2021; 258: 47-53. doi: 10.1016/j.jss.2020.08.040.
- Svensson K, Rolfson O, Mohaddes M, Malchau H, Erichsen Andersson A. Reflecting on and managing the emotional impact of prosthetic joint infections on orthopaedic surgeons: a qualitative study. Bone Joint J 2020 ; 102-b: 736-43. doi: 10.1302/0301-620x.102b6.Bjj-2019-1383.R1.
- Leta T H, Gjertsen J E, Dale H, Hallan G, Lygre S H L, Fenstad A M, et al. Antibiotic-loaded bone cement in prevention of periprosthetic joint infections in primary total knee arthroplasty: a register-based multicentre randomised controlled non-inferiority trial (ALBA trial). BMJ Open 2021 ; 11: e041096. doi: 10.1136/bmjopen-2020-041096.