High prevalence of patellar dislocation and trochlear dysplasia in a geographically and genetically isolated society: an observational national cohort study from the Faroese Knee Cohort
Niclas H EYSTUROY 1, Hans-Christen HUSUM 2, Elinborg S MORTENSEN 1, Lars BLØND 4, Per HÖLMICH 3, and Kristoffer W BARFOD 3
1 Department of Orthopedic Surgery, National Hospital of the Faroe Islands, Torshavn, the Faroe Islands; 2 Interdisciplinary Orthopedics, Aalborg University Hospital; 3 Sports Orthopedic Research Center – Copenhagen (SORC-C), Department of Orthopedic Surgery, Copenhagen University Hospital Amager-Hvidovre, Copenhagen; 4 Zealand University Hospital, Køge and Aleris Hospital, Copenhagen, Denmark
Background and purpose — We aimed to calculate the prevalence of patellar dislocation (PD) and trochlear dysplasia (TD) in a national cohort aged 15–19 years in the Faroe Island.
Patients and methods — All inhabitants in the Faroe Islands aged 15–19 years were invited to answer an online survey, including demographics and questions regarding prior PD. Participants with prior PD were invited for radiographs and MRI of both knees to be taken. Trochlear dysplasia was defined as one of the following: Dejour type A–D on radiographs, lateral trochlear inclination angle (LTI) < 11°, or trochlear depth < 3 mm on MRI.
Results — 3,749 individuals were contacted, 41 were excluded, and 1,638 (44%) completed the survey. 146 reported a prior PD (the PD cohort) and 100 accepted to participate and have radiographs and MRI taken of both knees (the clinical PD cohort), 76 of whom were diagnosed with TD. The national prevalence of PD was 8.9%. The national prevalence of symptomatic TD was 6.8%. The prevalence of TD in the clinical PD cohort was 76%. TD was bilateral in 78% of TD patients, but only 27% of patients with bilateral TD had PD in both knees.
Conclusion — The prevalence of PD in the Faroe Islands is found to be very high. The national prevalence of TD and the prevalence of TD in participants with prior PD is high, indicating a potential genetic influence.
Citation: Acta Orthopaedica 2024; 95: 14–19. DOI https://doi.org/10.2340/17453674.2024.35229.
Copyright: © 2024 The Author(s). This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (https://creativecommons.org/licenses/by-nc/4.0/), allowing third parties to copy and redistribute the material in any medium or format and to remix, transform, and build upon the material for non-commercial purposes, provided proper attribution to the original work.
Submitted: 2023-06-01. Accepted: 2023-12-14. Published: 2024-01-18.
Correspondence: nicey@ls.fo
NHE was the primary investigator, establishing the cohort, seeing patients in the outpatient clinic, and the author of the article. HCH was responsible for data handling and statistics. EM made it possible to conduct the investigation, organized the cohort establishment, and further contributed to the study by including patients in the outpatient clinic and being part of the in-house review process. HCH, EM, LB, NHE, and participated in design of the study and correction of the article. KB, the primary supervisor, was active in the whole process from idea to project, supervising NHE and being key factor in the in-house review process.
The authors would like to thank the radiological department of the Faroe Islands National Hospital for their work regarding radiographs and MRI, Óluva, the project secretary, Mildrid, Oddrún and colleagues in the outpatient clinic, and Jens Godik for technical support.
Handling co-editors: Li Felländer-Tsai and Philippe sWagner
Acta thanks Yasmin Denise Hailer and Per-Henrik Randsborg for help with peer review of this manuscript.
Patellar dislocation (PD) is a common injury constituting 3.3% of all knee injuries [1] and claimed to be more frequent and disabling than anterior cruciate ligament tears [2,3].
National incidence rates of PD vary from 7–77/100,000 person-years [4,5] with the highest incidence found in patients aged 10–17 years (108/100,000 person-years) [6]. The varying incidence rates could be due to differences in selected cohorts, differences in study design, and the lack of generally accepted definitions.
Although the etiology of patellar instability is multifactorial, the most significant predisposing factor for PD is trochlear dysplasia (TD) [7]. The true prevalence of TD in the general population is unknown. DeVries et al. [8] found a prevalence of approximately 10% by using ultrasound on skeletally mature adolescents and parents of patients (≤ 50 years of age) who presented to orthopedic clinic other than for knee problems. Dejour et al. [9] found the prevalence of TD in a cohort of 143 patients who had undergone surgery for recurrent PD to be 85%.
There is increasing evidence of a genetic contribution to PD and TD, with small studies reporting a familial association as a risk factor for the development of PD and TD [10], but no conclusion or deeper elaboration of the familial association has been described. The Faroe Islands form a geographically and genetically isolated country in the Atlantic Ocean where clinicians claim an abnormally high incidence of PD and TD. An accumulation of PD and TD in a genetically isolated society would argue for a genetic influence on the development of PD and TD.
There are no prior prospective national cohort studies reporting the prevalence of PD and TD in a general population. We aimed to calculate the prevalence of PD and TD in a national cohort in the Faroe Islands and compare with previously reported rates in genetically heterogeneous populations, and to investigate the demographic differences between the background population and the PD cohort, as well as the PD cohort with and without TD.
Patients and methods
Design and setting
The study was designed as a prospective national cohort study conducted in the Faroe Islands, a geographically small and genetically isolated country in the north of the Atlantic Ocean with 54,081 inhabitants as at October 4, 2021 [11]. The study report adheres to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement.
Study population
A national cohort was created by inviting all inhabitants of the Faroe Islands aged from 15 to the end of the 19th year to answer an online survey.
This age group was chosen to start at 15 years of age to avoid ethical problems and to ensure that the participants could answer the online survey independently. Also, most will already have experienced their first PD, and most will have mature bone morphology. Because many inhabitants leave the country to study abroad at around the age of 20, this age was chosen to be the upper age limit for the cohort.
The survey included basic demographics including age, sex, weight, height, sports, and smoking. Participants were asked if they had experienced PD, defined as an acute injury where the kneecap was sitting on the lateral side of the knee, causing immense pain and immobilization. An invitation to a personal online survey was sent to the inhabitants by secure personal email through the civil registration system in the Faroe Islands. If the email was not opened after 2 days, regular mail containing a direct personal link and QR code was sent. Non-responders received up to 3 invitations in the same manner described, with a 2-month interval.
Both those with and without prior knee problems were encouraged to answer the survey. Those who answered that they had had a prior PD were invited for a clinical examination, radiography, and MRI of both knees.
The whole cohort of participants answering the questionnaire constitute “The Faroese Knee Cohort (FKC).” The FKC is divided into 3 sub-cohorts: (1) the background cohort, consisting of the participants with no prior PD, (2) the PD cohort, consisting of participants with prior PD, (3) the clinical PD cohort, consisting of participants with prior PD who participated in the clinical and radiological follow-up.
The National Registry of the Faroe Islands identified 3,749 inhabitants as at October 4, 2021 [11] in the age group 15–19 years old (19 included).
41 individuals were excluded as they had left the country, leaving 3,708 eligible for inclusion in the cohort (Figure 1). 1,637 (44%) completed the survey, constituting the Faroese Knee Cohort. 1,491 reported no prior PD, constituting the Background Cohort. 146 reported prior PD, constituting the PD cohort. 100 accepted to participate in the clinical and radiological follow-up, constituting the Clinical PD cohort (Figure 1). In the Clinical PD cohort, 21 participants had unilateral MRI of the affected knee and no scan of the contralateral knee (5 participants did not give permission and 16 felt discomfort during scanning, thus the procedure was abandoned after scanning of the affected knee).
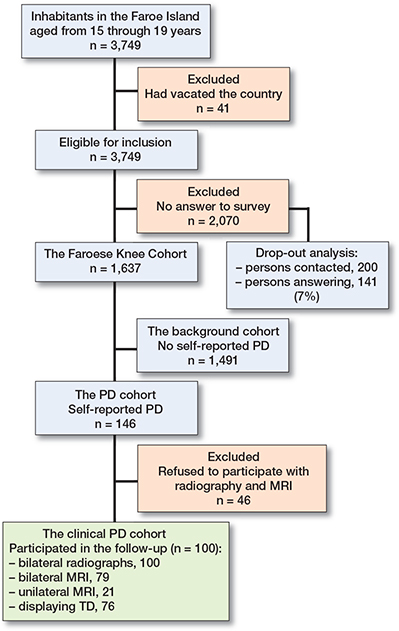
Figure 1. Flow diagram illustrating the establishment of the Faroese Knee Cohort and sub-cohorts. The Faroese knee cohort, consisting of all participants who answered the survey (n = 1,637), the PD cohort, consisting of all patients with self-reported PD (n = 146), and the clinical PD cohort, consisting of all patients with prior PD who underwent a clinical examination, radiography, and MRI of the knees. 21 participants in the clinical PD cohort had only unilateral MRI performed because 5 participants did not give permission and 16 felt discomfort during scanning, so the procedure was abandoned after scanning of the affected knee.
Study data was collected and managed using Research Electronic Data Capture (REDCap; https://www.project-redcap.org/) tools hosted at the National Hospital of the Faroe Islands [12,13]. REDCap is a secure, web-based software platform designed to support data capture for research.
Dropout analysis
To account for bias, a dropout analysis was conducted by contacting 10% of the non-responders by phone. A random list of 10% of the non-responders was created. The non-responders were contacted by phone and asked if they had experienced having a patellar dislocation as defined above.
Outcomes
PD was defined as already described. Participants were informed of this definition before answering the survey. During the visit to the outpatient clinic, all participants in the clinical PD cohort were interviewed by an orthopedic surgeon to validate the diagnosis.
TD should be seen as a continuum and the optimal measurement method and thresholds are debated [14]. Ultimately, TD depends on where one sets the threshold. In this study, TD was defined as having one or more of the following: Dejour type A–D, lateral trochlear inclination (LTI) < 11°, or a trochlear depth < 3 mm [15].
The Dejour classification was evaluated as described by Dejour et al. [16]. A true lateral projection radiograph was taken of both knees with the knee in 30° of flexion and the posterior aspects of the femoral condyles superimposed. To ensure high-quality true lateral projections, this was done using continuous radiographic imaging. If the crossing sign was present, the participant was said to have TD. The crossing sign is reproducible and simple to perform. The crossing sign has a sensitivity of 94% and a specificity of 56% [17] (Figure 2).
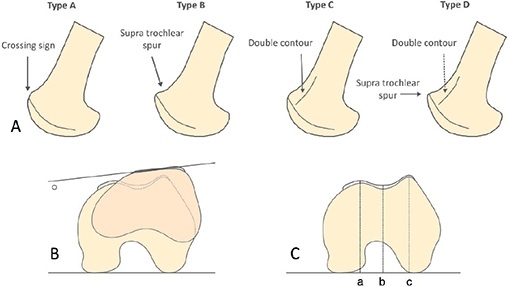
Figure 2. A. Dejour classification. The classification is performed on the true lateral radiographic projection of the knee. Type A is characterized by the crossing sign. Type B is characterized by the crossing sign and the supra-trochlear spur. Type C is characterized by the crossing sign and the double contour. Type D is characterized by the crossing sign with the supra-trochlear spur and the double contour. Modified from Creative Commons Attribution ©.
B. The lateral inclination angle is the angle between the most dorsal aspect of the posterior femoral condyles and the most proximal chondral surface of the lateral trochlear facet.
C. Trochlear depth is the outset depth of the trochlear groove (sulcus) relative to the mean of the medial and lateral femoral condyle outsets. Trochlear depth = (a+c)/2 – b.
The LTI [18] was measured on axial T1 MRI using the 2-image technique by Joseph et al. [19]. It measures the angle between the most dorsal aspect of the posterior femoral condyles and the most proximal chondral surface of the lateral trochlear facet. The mean value of LTI is reported to be 16.9° in knees without TD. Using a diagnostic threshold of 11°, the measure has shown a sensitivity of 93% and a specificity of 87% for TD in both skeletally mature and immature patients [18] (Figure 2).
The TD was measured on axial T1 MRI as defined by Pfirrmann et al. [20]. This measures the inset depth of the trochlear groove (sulcus) relative to the mean of the medial and lateral femoral condyle outsets. The measurement was done by drawing the tangent to the posterior aspect of both condyles as a reference baseline 3 cm proximal to the joint line. Perpendicular to this baseline, measurements were made to the most anterior points of the medial and lateral facets, as well as to the trochlear floor. The measurement was made relative to the cartilaginous (not osseous) surface of the trochlea. To compute the final metric, the floor measurement is subtracted from the average of the two facet measurements. A trochlear depth of < 3 mm is considered abnormal. The sensitivity is 100% and specificity is 96% in both skeletally mature and immature patients [21] (Figure 2).
The MRI scans were performed on a Siemens Magnetom Aera 1.5 Tesla gradient system (Siemens, Munich, Germany) with a TX/RX 15-channel knee coil. Measurements were done on axial T1-weighted proton density turbo spin echo, fat-suppressed (TR/TE 3390/32), field of view 16 cm, matrix size 256, number of excitations 2; slice thickness 3 mm sequences were used for measurements. The axial slice was defined as being perpendicular to the femoral axis in the frontal plane, and parallel to the posterior condyle line in the transverse plane.
Statistics
Normality of continuous data was checked by inspection of QQ plots. Continuous data is reported as mean and standard deviation (SD). Dichotomous data is reported as number (percentage). National prevalence of PD was calculated by number of cases (PD) divided by the proportion of total survey answers. The assumption of TD being as frequent in non-participants (those with prior PD but who did not wish to participate further in the study) as in participants (the clinical PD cohort) was made when calculating the national prevalence of TD. All patients investigated for TD had prior PD. The proportion who had TD was therefore divided by the total number of PD patients and then divided by the proportion of total survey answers. A Venn diagram was calculated for knees where both radiographs and MRI scans were available. Analyses were performed using Stata version 17.0 (StataCorp, College Station, TX, USA).
Ethics, registration, funding, data sharing, and disclosures
This study has been approved by the National Data Protection Agency of the Faroe Islands (Journal nr. 20/00178-6) and the Ethical committee of the Faroe Islands. This study is registered at Clinicaltrials.gov (ID: NCT04607538). Anonymized data is available upon request addressed to the first author if in accordance with the rules of the hospital and data protection legislation of the Faroe Islands. This research has been funded by the Research Council of the Faroe Islands. The authors have no conflict of interest to declare. Complete disclosure of interest forms according to ICMJE are available on the article page, doi: 10.2340/17453674.2024.35229
Results
All participants in the clinical PD cohort (n = 100) had bilateral radiographs of the knees. 79 had additional bilateral MRI and 21 had unilateral MRI scans performed, totaling 200 knee radiographs and 179 knee MRI scans for analysis (Figure 1).
Basic demographic data for the background cohort and the PD cohort is given in Table 1.
| Factor | PD cohort | Background cohort | Total |
| Number | 146 (8.9) | 1,491 (91) | 1,637 (100) |
| Sex | |||
| Female | 83 (57) | 738 (49) | 821 (50) |
| Male | 63 (43) | 753 (51) | 816 (50) |
| Age, mean (SD) | 17.9 (1.4) | 17.9 (1.4) | 17.9 (1.4) |
| Weight, mean (SD) | 73.2 (18.4) | 70.4 (15.3) | 70.7 (15.6) |
| Sports activity a | |||
| Active | 72 (50) | 879 (59) | 951 (58) |
| Inactive | 73 (50) | 611 (41) | 684 (42) |
| Hours of sports activity per week | |||
| 1–2 | 7 (9.7) | 48 (5.5) | 55 (5.8) |
| 2–5 | 21 (29) | 224 (26) | 245 (26) |
| 5–10 | 23 (32) | 382 (44) | 405 (43) |
| > 10 | 21 (29) | 221 (25) | 242 (26) |
| Pivoting sports b | |||
| No pivoting sport | 39 (31) | 372 (38) | 411 (37) |
| Pivoting sport | 86 (69) | 607 (62) | 693 (63) |
| Smoking status | |||
| Current/previous smoker | 29 (20) | 135 (9.1) | 164 (10) |
| Never smoked | 117 (80) | 1,354 (91) | 1,471 (90) |
| a Sports includes all answers. | |||
| b Among those who do sports. | |||
The national prevalence of PD was 146/1,637 (8.9%, 95% confidence interval [CI] 7.6–10.4). The prevalence of TD in the clinical PD cohort was 76% (CI 66–84). The national prevalence of symptomatic TD was 6.8% (CI 5.6–8.1).
Basic demographic data, age of first PD, number of PDs and prior injury of the knee from participants with or without TD in the clinical PD cohort is listed in Table 2.
| Factor | Trochlear dysplasia a | No trochlear dysplasia |
| Number | 76 | 24 |
| Height, cm | 172 (9.5) | 170 (6.8) |
| Weight, kg | 73.7 (17.5) | 70.7 (25.3) |
| Age at first dislocation | 13.7 (2.5) | 14.0 (2.4) |
| Number of dislocations | 4.5 (4.3) | 3.3 (3.7) |
| Prior knee injury, n (%) | 11 (14) | 5 (21) |
| a According to any definition. | ||
78% (CI 67–86) of participants with TD had bilateral TD, and of these 27% (CI 16–40) had bilateral PD.
The distribution of TD per knee according to Dejour, LTI, and trochlear depth is illustrated in Figure 3. Of the 179 knees available for all 3 measurements methods, 57 (32%) fulfilled all diagnostic criteria.

Figure 3. Distribution of trochlear dysplasia in the clinical PD cohort according to measurement per knee. Knees with both radiographs and MRI were included. 49 knees (27%) did not have trochlear dysplasia according to any of the 3 applied definitions. N = 179.
Dropout analysis
200 individuals were contacted and 141 answered the questions, representing 7% of the non-responders. Mean age was 17.9 (CI 17.7–18.2), 82 (58%, CI 50–-66) were male, and 3 (2.1%, CI 0.4–6.1) had prior self-reported ACL rupture. 11 in all reported prior PD (7.9%, CI 4.0–14).
Discussion
We aimed to calculate the prevalence of patellar dislocation (PD) and trochlear dysplasia (TD) in a national cohort aged 15–19 years in the Faroe Island. To the authors’ knowledge, we found the highest reported prevalence of PD reported in the literature to date. Further, the national prevalence of symptomatic TD was 6.8%, and 76% of patients with PD were diagnosed with TD.
Epidemiological studies in the Nordic countries report mean incidences of PD ranging from 42 to 77/100,000 person-years [4,6], with the highest incidence in young females (10–17 years) at 108/100,000 person-years [6]. A US military cohort showed an incidence of 69/100,000 person-years [5]. While these studies rely on ICD-code registrations, potentially leading to underestimation, our data, relying on self-reporting, is independent of registry accuracy. In comparison with the high rates in young females reported by Gravesen et al. [6], our study indicates an incidence approximately 7 times higher.
Reporting such a high prevalence of PD calls for reflection on correctness of data in our study. The high prevalence could indicate that the self-reported PD method either is better to find the true prevalence of PD, or gives an over-estimation due to misinterpretation of the question. However, participants in the clinical PD cohort were seen by an investigator in the outpatient clinic and the diagnosis of PD was confirmed; no participants were excluded due to misunderstanding of the PD diagnosis. On the contrary, patients with fast spontaneous reduction of the patella might not have reported prior PD.
The high prevalence of PD is credible, as it reflects the authors’ clinical experience of a proportional overrepresentation of patellar problems and total knee arthroplasties in Faroese patients, indicating an overrepresentation of knee pathology.
The Faroe Islands is both geographically and genetically isolated. Therefore, the risk of genetic inbreeding is high [26]. A high prevalence of any disease-causing phenotype, or skeletal abnormality, raises suspicion of a genetic etiology. There are several studies [27-29] indicating a familial accumulation of PD, but the studies have been undertaken with small populations, are of methodologically low and moderate quality, and without further elaboration of the familial association. Further studies are needed to determine whether familial association is a risk factor for PD [10].
The true prevalence of TD is unknown. In 1994, Dejour et al. [9] found trochlear dysplasia in 85% of 143 patients who had undergone patella-stabilizing surgery. This was done by measuring the crossing sign, the trochlear bump, and trochlear depth on radiographs and CT scans. In comparison, in the present cohort we found only 48% of patients with TD using the Dejour crossing sign. Using the wider criteria for TD (Dejour crossing sign, LTI, and trochlear depth), we found 76% with TD.
We investigated patients with a history of PD to determine the national prevalence of symptomatic TD. Given the likelihood of asymptomatic TD in the background population, the overall prevalence (symptomatic and asymptomatic cases) may exceed the numbers reported in this study. Comparisons with the Onor or DeVries studies may be limited. Notably, DeVries’s cohort includes individuals with severe clinical symptoms who underwent patella-stabilizing surgery.
We used the 2-image technique to measure LTI on MRI, with a diagnostic threshold of 11° [18], because it is most frequently used in the literature. The 2-image technique was found to be more reliable and sensitive by Joseph et al. [19], and this helped to avoid underrepresentation of TD, although Cheng et al. [22] suggested a threshold of 8.9° to achieve good discrimination between patients with and without patellar instability.
We chose to use the crossing sign, LTI, and trochlear depth measurements to avoid underestimation of the prevalence of TD, and also to have a method applicable for the skeletally immature population (LTI and trochlear depth). The 3 measurement methods have not been combined in earlier studies and could partially explain the high prevalence of TD in this study.
Finally, another interesting finding was that 78% of TD was bilateral, but only 27% had bilateral PD. The TD was equally severe according to the crossing sign on the dislocated side as on the contralateral side. Even though TD is the biggest risk factor for PD [7], this finding could be explained by the fact that a triggering trauma in most patients is necessary before the patella/knee becomes dysfunctional, reflecting the fact that 2/3 of primary acute PD occurs during pivoting sports [25]. This correlates to this cohort, as 2/3 of all participants reported their primary PD occurred during pivoting sports.
Strengths and limitations
It is a strength of this study that it is a prospective national cohort study with standardized radiography and MRI. It is the authors’ belief that self-reporting PD is a strength in this study, avoiding bias in the lack of hospital registration. However, self-reporting PD could also constitute a bias.
It is a weakness of this study that only 44% answered the survey. However, the dropout analysis found the average prevalence of PD among those who did not answer the survey to be very close to the participants in the survey.
Conclusion
The prevalence of PD (8.9%) in our study population from the Faroe Islands is markedly higher than reported in other studies conducted in larger countries with genetically heterogeneous populations, indicating that genetics may influence the development of PD and TD. 76% of patients with PD had TD, giving a national prevalence of TD of 6.8%. Most patients (78%) with TD in one knee exhibited the same pathology in the opposite knee, further indicating a genetic etiology to TD. A genealogical investigation of patients with PD and TD is warranted.
- Majewski M, Susanne H, Klaus S. Epidemiology of athletic knee injuries: a 10-year study. Knee 2006; 13(3): 184-8. https://doi.org/10.1016/j.knee.2006.01.005.
- Magnussen R A, Verlage M, Stock E, Zurek L, Flanigan D C, Tompkins M, et al. Primary patellar dislocations without surgical stabilization or recurrence: how well are these patients really doing? Knee Surg Sports Traumatol Arthrosc 2017; 25(8): 2352-6. https://doi.org/10.1007/s00167-015-3716-3.
- Straume-Næsheim T M, Randsborg P H, Mikaelsen J R, Sivertsen E A, Devitt B, Granan L P, et al. Recurrent lateral patella dislocation affects knee function as much as ACL deficiency: however patients wait five times longer for treatment. BMC Musculoskelet Disord 2019; 20(1). https://doi.org/10.1186/s12891-019-2689-7.
- Sillanpää P, Mattila V M, Iivonen T, Visuri T, Pihlajamäki H. Incidence and risk factors of acute traumatic primary patellar dislocation. Med Sci Sports Exerc 2008; 40(4): 606-11. https://doi.org/10.1249/MSS.0b013e318160740f.
- Hsiao M, Owens B D, Burks R, Sturdivant R X, Cameron K L. Incidence of acute traumatic patellar dislocation among active-duty United States military service members. Am J Sports Med 2010; 38(10): 1997-2004. https://doi.org/10.1177/0363546510371423.
- Gravesen K S, Kallemose T, Blønd L, Troelsen A, Barfod K W. High incidence of acute and recurrent patellar dislocations: a retrospective nationwide epidemiological study involving 24,154 primary dislocations. Knee Surg Sports Traumatol Arthrosc 2018; 26(4): 1204-9. https://doi.org/10.1007/s00167-017-4594-7.
- Steensen R N, Bentley J C, Trinh T Q, Backes J R, Wiltfong R E. The prevalence and combined prevalences of anatomic factors associated with recurrent patellar dislocation: a magnetic resonance imaging study. Am J Sports Med 2015; 43(4): 921-7. https://doi.org/10.1177/0363546514563904.
- DeVries C A, Bomar J D, Pennock A T. Prevalence of trochlear dysplasia and associations with patellofemoral pain and instability in a skeletally mature population. J Bone Joint Surg Am 2021; 103(22): 2126-32. https://doi.org/10.2106/JBJS.20.01624.
- Dejour H, Walch G, Nove-Josserand L, Guier C. Factors of patellar instability: an anatomic radiographic study. Knee Surg Sports Traumatol Arthrosc 1994; 2(1): 19-26. https://doi.org/10.1007/BF01552649.
- Danielsen O, Poulsen T A, Eysturoy N H, Mortensen E S, Hölmich P, Barfod K W. Familial association and epidemiological factors as risk factors for developing first time and recurrent patella dislocation: a systematic review and best knowledge synthesis of present literature. Knee Surg Sports Traumatol Arthrosc 2023; 31(9): 3701-33. https://doi.org/10.1007/s00167-022-07265-z.
- Statistics of the Faroe Island Population [Internet]. [cited 2023 Jan 23]. https://hagstova.fo/en/population/population/population (accessed January 23, 2023).
- Harris P A, Taylor R, Minor B L, Elliott V, Fernandez M, O’Neal L, et al. The REDCap consortium: building an international community of software platform partners. J Biomed Inform 2019; 95: 103208. doi: 10.1016/j.jbi.2019.103208.
- Harris P A, Taylor R, Thielke R, Payne J, Gonzalez N, Conde J G. Research electronic data capture (REDCap): a metadata-driven methodology and workflow process for providing translational research informatics support. J Biomed Inform 2009; 42(2): 377-81. https://doi.org/10.1016/j.jbi.2008.08.010.
- Paiva M, Blønd L, Hölmich P, Steensen R N, Diederichs G, Feller J A, et al. Quality assessment of radiological measurements of trochlear dysplasia; a literature review. Knee Surg Sports Traumatol Arthrosc 2018; 26(3): 746-55. https://doi.org/10.1007/s00167-017-4520-z.
- Paiva M, Blønd L, Hölmich P, Steensen R N, Diederichs G, Feller J A, et al. Quality assessment of radiological measurements of trochlear dysplasia: a literature review. Knee Surg Sports Traumatol Arthrosc 2018; 26(3): 746-55. https://doi.org/10.1007/s00167-017-4520-z.
- Dejour H, Walch G, Neyret P, Adeleine P. [Dysplasia of the femoral trochlea]. Rev Chir Orthop Reparatrice Appar Mot 1990; 76(1): 45-54.
- Batailler C, Neyret P. Trochlear dysplasia: imaging and treatment options. EFORT Open Rev [Internet] 2018; 3(5): 240-7. https://doi.org/10.1302/2058-5241.3.170058.
- Carrillon Y, Abidi H, Dejour D, Fantino O, Moyen B, Tran-Minh V A. Patellar instability: assessment on MR images by measuring the lateral trochlear inclination: initial experience. Radiology 2000; 216(2): 582-5. doi: 10.1148/radiology.216.2.r00au07582.
- Joseph S M, Cheng C, Solomito M J, Pace J L. Lateral trochlear inclination angle: measurement via a 2-image technique to reliably characterize and quantify trochlear dysplasia. Orthop J Sports Med 2020; 8(10): 10.1177/2325967120958415. https://doi.org/10.1177/2325967120958415.
- Pfirrmann C W, Zanetti M, Romero J, Hodler J. Femoral trochlear dysplasia: MR findings. Radiology 2000; 216(3): 858-64. https://doi.org/10.1148/radiology.216.3.r00se38858.
- Stepanovich M, Bomar J D, Pennock A T. Are the current classifications and radiographic measurements for trochlear dysplasia appropriate in the skeletally immature patient? Orthop J Sports Med 2016; 4(10). https://doi.org/10.1177/2325967116669490.
- Cheng C, Hedgecock J, Solomito M, Joseph S, Pace J L. Defining trochlear dysplasia via the lateral trochlear inclination angle. Orthop J Sports Med 2020; 8(4_suppl3): 2325967120S0017. https://doi.org/10.1177/2325967120s00179.
- Köhlitz T, Scheffler S, Jung T, Hoburg A, Vollnberg B, Wiener E, et al. Prevalence and patterns of anatomical risk factors in patients after patellar dislocation: a case control study using MRI. Eur Radiol 2013; 23(4): 1067-74. https://doi.org/10.1007/s00330-012-2696-7.
- Onor G I, Yalcin S, Kaar S G, Pace J L, Ferrua P, Farrow L D. The evaluation of trochlear osseous morphology: an epidemiologic study. Orthop J Sports Med 2021; 9(4): 2325967121994548. https://doi.org/10.1177/2325967121994548.
- Lyons J G, Hudson T L, Krishnamurthy A B. Epidemiology of patellar dislocations in the United States from 2001 to 2020: results of a National Emergency Department database. Phys Sportsmed 2022; Online ahead of print. https://doi.org/10.1080/00913847.2022.2156765.
- Mortensen Ó, Thomsen E, Lydersen L N, Apol K D, Weihe P, Steig B, et al. FarGen: elucidating the distribution of coding variants in the isolated population of the Faroe Islands. Eur J Hum Genet 2023; 31(3): 329-37. https://doi.org/10.1038/s41431-022-01227-2.
- Smith T O, Donell S T, Chester R, Clark A, Stephenson R. What activities do patients with patellar instability perceive makes their patella unstable? Knee 2011; 18(5): 333-9. https://doi.org/10.1016/j.knee.2010.07.003.
- Atkin D M, Fithian D C, Marangi K S, Stone M L, Dobson B E, Mendelsohn C. Characteristics of patients with primary acute lateral patellar dislocation and their recovery within the first 6 months of injury. Am J Sports Med 2000; 28(4): 472-9.doi: 10.1177/03635465000280040601.
- Fithian D C, Paxton E W, Stone M L, Silva P, Davis D K, Elias D A, et al. Epidemiology and natural history of acute patellar dislocation. Am Sports Med 2004; 32(5): 1114-21. https://doi.org/10.1177/0363546503260788.