Girdlestone resection arthroplasty for femoral neck fractures has poorer outcomes than hemiarthroplasty in frail patients with increased risk for arthroplasty-related complications: a retrospective case study of 21 patients
Petri BELLOVA, Marcus LINNE, Anne Elisabeth POSTLER, Klaus-Peter GÜNTHER, Maik STIEHLER, and Jens GORONZY
Department of Orthopaedics, Trauma and Plastic Surgery, University Clinic Garl Gustav Carus, Technical University (TU) Dresden, Germany
Abstract
Background and purpose — Hemiarthroplasty (HA) is the usual treatment for displaced femoral neck fractures (FNF) in elderly patients. Patients may be unsuitable for HA due to secondary conditions such as systemic infections or severe neurological conditions, which is why Girdlestone resection arthroplasty (GRA) may be an option. We aimed to determine (1) patient survival in matched patient groups treated with either GRA or HA and (2) functional outcomes.
Patients and methods — 21 patients treated with GRA for FNF in a German university hospital were retrospectively reviewed (2015–2019). After matching for age and comorbidities, a control group of 42 HA patients was established. Patient survival was determined by a Kaplan–Meier analysis. The mean follow-up (FU) was 1.5 (0–4.4) years. Function at FU was documented using the modified Harris Hip Score (mHHS) and the National Hip Fracture Database (NHFD) mobility score.
Results — The 1-month-mortality was 19% in the GRA group and 12% in the HA group; the 1-year mortality was 71% and 49%, respectively (P = 0.01). The mHHS at FU was lower in the GRA group than in the HA group (22 [range 0–50] vs. 46 [11–80]). 82% of patients in the GRA group were bedridden post-surgery as opposed to 19% in the HA group.
Conclusion — Patients with HA after FNF had higher survival and better functional outcomes when compared with GRA in matched patient groups. Considering this, GRA for FNF should be selected restrictively.
Citation: Acta Orthopaedica 2024; 95: 61–66. DOI https://doi.org/10.2340/17453674.2024.34901.
Copyright: © 2024 The Author(s). This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (https://creativecommons.org/licenses/by-nc/4.0/), allowing third parties to copy and redistribute the material in any medium or format and to remix, transform, and build upon the material for non-commercial purposes, provided proper attribution to the original work.
Submitted: 2023-03-20. Accepted: 2023-11-23. Published: 2024-01-30.
Correspondence: petri.bellova@uniklinikum-dresden.de
PB, ML, and JG initiated and designed the study and managed the ethical review board application. PB and ML performed the statistical analyses and drafted the manuscript. AEP, MS, KPG, and JG took part in data analysis and editing. All authors gave their final approval of the version submitted.
The authors would like to acknowledge Franziska Beyer and Anne Schützer from our department’s study group for assisting with the statistical analysis.
Handling co-editors: Cecilia Rogmark and Philippe Wagner
Acta thanks Camilla Bergh and Bjarke Viberg help with peer review of this manuscript.
The preferred treatment option for displaced fractures in elderly patients is hemiarthroplasty, (HA) as it can alleviate pain and restore early postoperative mobility [1]. However, coexisting conditions such as systemic infections, pressure sores, or severe neurological conditions such as dementia and Parkinson’s disease are associated with an increased risk of periprosthetic joint infection (PJI), dislocation, or other arthroplasty-related complications and may keep treating surgeons from choosing arthroplasty. Alternatives to HA in these patients include nonoperative management (NOM), internal fixation, or Girdlestone resection arthroplasty (GRA).
In 1928, Girdlestone [2] described extensive excision arthroplasty of the hip as a salvage procedure for tuberculous arthritis. Today the acronym GRA is used for head–neck resection or implant removal and mostly used in the treatment of PJI.
GRA used as the primary treatment of patients with FNF is a rather rarely mentioned treatment option and is only described in a few small studies [3-5].
We aimed to determine (1) patient survival of matched cohorts treated with either GRA or HA as primary treatment of FNF and (2) functional outcomes of the 2 groups.
Patients and methods
This is a retrospective matched cohort study on FNF patients treated with GRA due to a potentially increased risk of arthroplasty-related complications. The reporting adheres to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement [6]. The study was conducted in a single center.
All patients with FNF in the recruitment period January 2015–December 2019 were reviewed for this study and those treated with HA or GRA were isolated for further analysis. As data was collected within a given time period, and cases were few, a study size calculation was not made. The follow-up (FU) was conducted in June 2021 (1.5 years after the last inclusion). The department had no clear guidelines for the GRA indication but the rationales for choosing GRA were mainly that a patient was very frail with concomitant systemic infections or had neurological disorders and limited pre-injury mobility. All GRA patients were included in the study except for patients with pathological FNF (Figure 1).
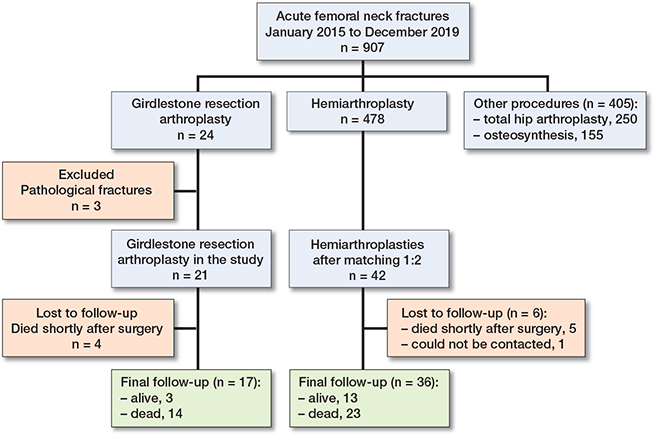
Figure 1. Flowchart of patient inclusion.
2 HA patients were allocated to each GRA patient according to a matching process including matching criteria in the following priority order:
- American Society of Anesthesiologists (ASA) score (identical).
- Charlson Comorbidity Index (CCI) ± 1 point.
- Age at surgery ± 3 years.
- Date of surgery ± 3 months.
If more than 2 HA cases fulfilled the matching criteria, the 2 patients with the most similar characteristics were selected. If fewer than 2 HA cases fulfilled the criteria (n = 4), the inclusion criteria were sequentially dropped in reverse order (first “date of surgery ± 3 months”, then “age at surgery ± 3 years”). All matching partners at least fulfilled the ASA and CCI criteria.
Surgical procedure
GRA was performed using a direct lateral approach. After exposure through a T-shaped capsulotomy, a femoral neck osteotomy with an oscillating saw was performed and the femoral head was extracted. After thorough jet lavage of the situs, a drain was placed in the joint and layerwise closure was performed.
HA was performed using the same approach as described above. The stem anchorage was acheived using a 3rd-generation cementation technique, followed by the insertion of the bipolar head and joint reduction.
All reported surgery-related and medical complications (Table 2) occurred during the initial in-hospital care of patients.
Follow-up
The FU consisted of a postal questionnaire and/or telephone interview, which could be answered by patients or their proxies. The FU included the National Hip Fracture Database (NHFD) mobility score with “1” indicating the best possible and “5” the worst possible mobility, a modified Harris Hip Score (mHHS) [7] considering only the sections for pain and functionality extrapolated together to 100 points, as well as the Euroqol-5-dimensions 5 levels (EQ- 5D-5L) [8] score. Permission to use the EQ- 5D-5L for non-commercial use was obtained via www.euroqol.org. Patient satisfaction was questioned on a scale from 1 (extremely dissatisfied) to 100% (extremely satisfied). FU time was defined as the time between surgery and the FU or between surgery and death in deceased patients.
If patients were unable to actively participate due to, e.g., severe dementia or hearing difficulties, proxies or close relatives answered on their behalf. The variables at FU were obtained irrespective of whether the patients were alive or not. In the case of death, we recorded the best status reached by patients at any time after surgery.
Statistics
The survival analysis was performed using the Kaplan–Meier method. The endpoint was patient death from any cause. A log rank test was performed to determine the difference between the 2 groups. The P value of the test was given at a significance level of α = 5%. The median survival of the groups was determined and presented with the 95% confidence interval (CI) in parentheses. Secondary outcome variables included patient functionality using the scores mentioned previously. Categorical variables were presented as counts with percentages in parentheses, continuous variables as mean with the range in parentheses. The statistical analysis was conducted using SPSS v. 27 (IBM Corp, Armonk, NY, USA).
Ethics, funding, and potential conflicts of interest
Prior to study initiation, approval by the local ethics committee was obtained (trial registration ID “BO-EK-254062020”). Informed consent was obtained from all study participants. No competing interests were declared by any of the authors. Complete disclosure of interest forms according to ICMJE are available on the article page, doi: 10.2340/17453674.2024.34901
Results
907 patients with FNF were admitted to our hospital in the recruitment period. 478 patients (53%) received HA, while 250 patients (28%) received total hip arthroplasty. 155 patients (17%) were treated by internal fixation and 24 patients by GRA (2.7%). Of these, 3 patients with pathological FNF were excluded, leaving 21 patients in the GRA group for further consideration (Figure 1).
17 GRA patients and 36 HA patients were followed up (Figure 1). In 4 GRA patients, no FU status could be obtained because these patients had died shortly after surgery. 6 HA patients were lost to FU and excluded from the final analysis: 5 had died shortly after surgery and 1 could not be contacted.
The mean FU time for patients included in this study (n = 53) was 1.5 (0–4.4) years. The mean FU time for GRA patients (n = 17) was 0.8 (0–3.2) years and for HA patients (n = 36) 1.8 (0–4.4) years. The mean FU time for patients who were still alive at FU was 1.8 (1.5–2.0) years in the GRA group (n = 3) and 2.9 (1.5–4.4) years in the HA group (n = 15).
Baseline characteristics
Age at surgery was 79 (63–98) years in the GRA and 81 (64–96) years in the HA group. The mean CCI was 7.1 (3–13) and 7.1 (4–12) while the mean ASA score was 3.0 (1–4) and 3.1 (2–4) in the GRA and HA groups, respectively. The preoperative ambulatory status was similarly distributed in both groups ( Table 1).
Survival (Figure 2)
Survival after 1 month was 81% in the GRA and 88% in the HA group and 29% and 51% after 12 months, respectively. The median survival was 3.3 (CI 0–6.8) months in the GRA and 15.9 (CI 3.9–27.9) months in the HA group (χ² = 6.6; P = 0.01).
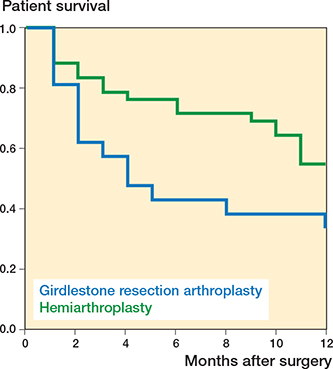
Figure 2. Kaplan–Meier survival analysis depicting Girdlestone resection arthroplasty group (blue curve) and hemiarthroplasty group (green curve). Survival was 81% in the GRA versus 88% in the HA group after 1 month, and 29% versus 51% after 12 months, respectively (log rank: P = 0.01).
At the final FU, 18 of the 21 patients in the GRA group had died while in the HA group, 26 of 42 had died. Among the deceased, death had occurred after a mean of 0.6 (0–3.2) years postoperatively in the GRA group and after a mean of 0.8 (0–3.7) years postoperatively in the HA group.
The mean surgery duration was 42 (14–68) minutes in the GRA group and 84 (54–161) minutes in the HA group (Table 2). Among the GRA patients, none had surgery-related complications. Among patients treated by HA, one patient was converted to a dual-mobility implant due to recurrent dislocation. Another suffered an intraoperative periprosthetic fracture of the greater trochanter, which was treated conservatively with partial weightbearing. 3 patients had prolonged wound drainage but none of them had to be revised.
10 GRA patients and 12 HA patients had medical complications (Table 2). Of the 10 GRA patients, 2 died during their hospital stay due to the sequelae of these complications, 1 following pneumonia with ensuing sepsis and 1 due to the sequelae of a urogenital tumor.
Function
Both the mHHS and the EQ-5D were decreased in the GRA group (Table 3). Patient satisfaction was 37% (0–90) in the GRA group and 67% (20–100) in the HA group.
14 of 17 patients (82%) in the GRA group were bedridden at FU (NHFD V) as opposed to 7 of 36 (20%) in the HA group. 19 of the HA patients were mobile within their home (NHFD IV); 7 could walk outside with walking aids (NHFD III).
2 GRA patients received secondary arthroplasty; 1 patient was still alive at the final FU while the other had died 5 years after arthroplasty was performed.
Discussion
The aim of the study was to evaluate GRA as a potential treatment alternative for FNF in very frail patients with concomitant infections or other conditions that might lead surgeons to decide against arthroplasty. In matched patient groups of GRA and HA patients we found a higher 1-year mortality after GRA. Also, function was impaired to a higher degree following GRA when compared with HA.
Because GRA is rarely used as a primary treatment option for FNF, only limited literature on GRA exists. In most western nations, as in Germany, HA is usually the preferred treatment for FNF even in very frail patients, as it is also considered as a palliative care approach to minimize pain and other symptoms. HA can be regarded as unsuitable for some patients due to concomitant systemic infections, or limited mobility or life expectancy. In these special circumstances NOM [9] or— more rarely—GRA can be discussed.
A hip fracture is associated with increased all-cause mortality and patients with hip fractures may have a 3-fold higher mortality compared with the general population [10,11]. In a large Danish population study, 1-year-mortality after hip fracture was 27% [12]. In certain patient groups mortality rates can be even higher, such as in patients with dementia [13]. In our GRA group, 1-year mortality was 71%. A lower 1-year mortality than ours, with rates of 28 and 27%, respectively, was reported in 2 studies where GRA was used after a hip fracture but mainly after complications of hip arthroplasty [14,15]. A study reporting on GRA primarily used for FNF in relatively young patients (57 years) found a 21% mortality after 5 years [4]. Also, major comorbidities at least were not reported, thus representing a different selection from ours. More in line with our study, Shah and Parker [3], investigating GRA as a primary or secondary procedure for a hip fracture, found a 1-year mortality of 42%. However, a majority received GRA secondary to complications of surgery.
Patients with FNF treated nonoperatively had 30-day and 1-year mortality rates for NOM of 87% and 99%, respectively, when compared with 7% and 28%, respectively, for surgery [16]. Other studies have displayed wider mortality ranges; a meta-analysis reported 30-day and 1-year mortality rates between 5% and 65% (36% average) and 30% and 95% (60% average), respectively [17]. Differences in mortality in the latter meta-analysis were, in particular, due to fundamental differences in patient characteristics between the studies. Patient selection may also explain the variation in mortality rates in all the above-cited studies.
Our results are supported by studies reporting limited mobility and a need for assistance after GRA, while results on pain relief are rather mixed [14,15,18]. In a group of 14 patients treated with GRA after neglected FNF, none of the 14 patients were taking regular pain medication and all could walk short distances, some with and some without walking aids at FU [4]. In 6 non-ambulatory patients receiving GRA for FNF, reduced pain scores pre- vs. postoperatively as well as restored baseline function were found [5]. In 36 patients treated with GRA mostly as a secondary procedure for a hip fracture, the mobility status for all patients had deteriorated compared with that before the fracture and 63% were immobile and unable to walk even with aids and assistance [3].
Regarding HA, Chammout et al. and Mouzopoulos et al. [19,20] reported functional outcomes (HHS; EQ-5D) that were slightly better than ours; however, in study groups with a presumably healthier case mix.
In NOM for FNF patients, mobility has been shown to be rather poor, with most patients bedridden or only able to perform basic bed–chair mobilization [21-23]. Again, NOM may be a more relevant comparator. Studies reporting on pain after NOM have displayed heterogeneous results. While Moulton et al. [21] found a majority of patients to be pain-controlled with analgesia at hospital discharge, other studies have reported poorer pain control with NOM [24].
Limitations
First, this is a retrospective study with missing or incorrect data due to previous poor recordkeeping as well as misclassification or information bias. Second, while we were able to match the 2 groups according to conventional comorbidity scores, we could not match them according to other crucial criteria that influenced the intervention. Among these, preoperative function would have been a desirable variable for matching, but it was not reliably documented and reproducible retrospectively. Furthermore, matching according to CRP values, the incidence of pressure sores, or active infections was also not achievable since these conditions had occurred very rarely in the HA group. This selection bias was a possible predictor for the poorer GRA outcomes. Of note, while age was a matching criterion, there was a large age variety in both groups (63–98) as prematurely aged patients with, e.g., neurological diseases resulting in a high degree of frailty were also included.
Third, because many patients were very frail, had cognitive impairment, or had died before FU, their proxies were often left to respond to the questionnaires on the patients’ behalf, which could have led to recall bias. Preoperative function was often unknown and could not be reliably compared with the postoperative status. Fourth, patients neither regularly underwent surgery within 24 hours at the time of this investigation, nor did they regularly receive targeted physiotherapy and geriatric co-management. These factors have been implemented recently and might have a significant influence on patient morbidity and mortality and possibly also on decision-making.
Strengths
This is the largest study on GRA exclusively as a primary treatment for FNF and the only study comparing the outcomes of GRA vs. HA in critically ill, elderly patients with FNF. Furthermore, a rather homogeneous group of frail patients was reviewed, who were selected by specific matching criteria.
When planning the treatment of a displaced FNF in a very frail patient, in particular in combination with a severe ongoing infection, the surgeon might consider different treatment options. The first option is to perform HA while simultaneously treating the infection. It may be perceived as risky, but this option probably presents the best chance for patients to regain mobility. The second option is NOM, which can be justified in a palliative setting, when the patient is life-threateningly ill, does not wish to prolong life, or declines surgery. Given correct implementation, pain levels can be kept low and functional results can be satisfactory [17,25]. However, as NOM is a palliative approach with a high short-term mortality, patients, their proxies, and healthcare professionals all need to be involved in the decision-making process. The third option is GRA, which might be considered in patients fit enough for surgery but with high risk of prosthesis-related complications. However, as shown by our results, the poor outcomes might speak in favor of other options even in these situations. From a clinical perspective, shared decision-making protocols can help to find the best individualized treatment for very frail FNF patients.
Conclusion
Patients with HA after FNF had higher survival and better functional outcomes when compared with GRA in matched patient groups.
GRA has been considered as an alternative treatment method for FNF, especially in frail or immobile patients with a concomitant severe ongoing infection. However, our study results suggest that GRA is associated with higher short-term mortality as well as with poorer functional results when compared with HA and should therefore be chosen restrictively as the primary treatment for FNF. However, due to the descriptive nature of this study, our findings may have limited generalizability.
- Rogmark C, Leonardsson O. Hip arthroplasty for the treatment of displaced fractures of the femoral neck in elderly patients. Bone Joint J 2016; 98-B(3): 291-7. doi: 10.1302/0301-620X.98B3.36515.
- Girdlestone G R. Arthrodesis and other operations for tuberculosis of the hip. In: Milford H, editor. The Robert Jones birthday volume. London, UK: Oxford University Press; 1928. pp: 347-74.
- Shah N, Parker M J. What is the outcome after a Girdlestone resection arthroplasty following a hip fracture? Hip Int 2023; 33(5): 948-51. doi: 10.1177/11207000221126135.
- Sawadogo M, Kafando H, Ouedraogo S, Korsaga A S, Ouedraogo S, Tinto S, et al. Is head and neck resection of the femur (Girdlestone’s procedure) still relevant? Indications and results about 24 cases. Open Orthop J 2018; 12: 69-74. doi: 10.2174/1874325001812010069.
- Steelman K, Bolz N, Fleming J, Vaidya R. Hip resection arthroplasty for acute femoral neck fractures in the non-ambulator. OTA Int 2022; 5(1): e167. doi: 10.1097/OI9.0000000000000167.
- Elm E v., Altman D G, Egger M, Pocock S J, Gøtzsche P C, Vandenbroucke J P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. Lancet 2007; 370(9596): 1453-7. doi: 10.1016/S0140-6736(07)61602-X.
- Harris W H. Traumatic arthritis of the hip after dislocation and acetabular fractures: treatment by mold arthroplasty. An end-result study using a new method of result evaluation. J Bone Joint Surg Am 1969; 51(4): 737-55.
- Herdman M, Gudex C, Lloyd A, Janssen M F, Kind P, Parkin D, et al. Development and preliminary testing of the new five-level version of EQ-5D (EQ-5D-5L). Qual Life Res 2011; 20(10): 1727-36. doi: 10.1007/s11136-011-9903-x.
- Sharma H, Kakar R. Outcome of Girdlestone’s resection arthroplasty following complications of proximal femoral fractures. Acta Orthop Belg 2006; 72(5): 555-9. PMID: 17152418
- Katsoulis M, Benetou V, Karapetyan T, Feskanich D, Grodstein F, Pettersson-Kymmer U, et al. Excess mortality after hip fracture in elderly persons from Europe and the USA: the CHANCES project. J Intern Med 2017; 281(3): 300-10. doi: 10.1111/joim.12586.
- Panula J, Pihlajamäki H, Mattila V M, Jaatinen P, Vahlberg T, Aarnio P, et al. Mortality and cause of death in hip fracture patients aged 65 or older: a population-based study. BMC Musculoskelet Disord 2011; 12: 105. doi: 10.1186/1471-2474-12-105.
- Jantzen C, Madsen C M, Lauritzen J B, Jørgensen H L. Temporal trends in hip fracture incidence, mortality, and morbidity in Denmark from 1999 to 2012. Acta Orthop 2018; 89(2): 170-6. doi: 10.1080/17453674.2018.1428436.
- Rajeev A, Ali M, Tuinebreijer W, Zourob E, Anto J. Preexisting dementia is associated with higher mortality rate in patients with femoral neck fracture. Aging Med (Milton) 2021; 4(1): 12-18. doi: 10.1002/agm2.12142.
- van der Zwaard B C, Stein C E, Bootsma J E M, van Geffen H J A A, Douw C M, Keijsers C J P W. Fewer patients undergo surgery when adding a comprehensive geriatric assessment in older patients with a hip fracture. Arch Orthop Trauma Surg 2020; 140(4): 487-92. doi: 10.1007/s00402-019-03294-5.
- Sharma H, Leeuw J de, Rowley D I. Girdlestone resection arthroplasty following failed surgical procedures. Int Orthop 2005; 29(2): 92-5. doi: 10.1007/s00264-004-0633-3.
- Wijnen H H, Schmitz P P, Es-Safraouy H, Roovers L A, Taekema D G, van Susante J L C. Nonoperative management of hip fractures in very frail elderly patients may lead to a predictable short survival as part of advance care planning. Acta Orthop 2021; 92(6): 728-32. doi: 10.1080/17453674.2021.1959155.
- Loggers S A I, van Lieshout E M M, Joosse P, Verhofstad M H J, Willems H C. Prognosis of nonoperative treatment in elderly patients with a hip fracture: a systematic review and meta-analysis. Injury 2020; 51(11): 2407-13. doi: 10.1016/j.injury.2020.08.027.
- Basu I, Howes M, Jowett C, Levack B. Girdlestones excision arthroplasty: current update. Int J Surg 2011; 9(4): 310-13. doi: 10.1016/j.ijsu.2011.01.012.
- Chammout G, Muren O, Bodén H, Salemyr M, Sköldenberg O. Cemented compared to uncemented femoral stems in total hip replacement for displaced femoral neck fractures in the elderly: study protocol for a single-blinded, randomized controlled trial (CHANCE-trial). BMC Musculoskelet Disord 2016; 17(1): 398. doi: 10.1186/s12891-016-1253-y.
- Mouzopoulos G, Stamatakos M, Arabatzi H, Vasiliadis G, Batanis G, Tsembeli A, et al. The four-year functional result after a displaced subcapital hip fracture treated with three different surgical options. Int Orthop 2008; 32(3): 367-73. doi: 10.1007/s00264-007-0321-1.
- Moulton L S, Green N L, Sudahar T, Makwana N K, Whittaker J P. Outcome after conservatively managed intracapsular fractures of the femoral neck. Ann R Coll Surg Engl 2015; 97(4): 279-82. doi: 10.1308/003588415X14181254788809.
- Rashidifard C H, Romeo N M, Muccino P, Richardson M, DiPasquale T G. Palliative management of nonoperative femoral neck fractures with continuous peripheral pain catheters: 20 patient case series. Geriatr Orthop Surg Rehabil 2017; 8(1): 34-8. doi: 10.1177/2151458516683226.
- Lim W X, Kwek E B K. Outcomes of an accelerated nonsurgical management protocol for hip fractures in the elderly. J Orthop Surg (Hong Kong) 2018; 26(3): 2309499018803408. doi: 10.1177/2309499018803408.
- Berry S D, Rothbaum R R, Kiel D P, Lee Y, Mitchell S L. Association of clinical outcomes with surgical repair of hip fracture vs non-surgical management in nursing home residents with advanced dementia. JAMA Intern Med 2018; 178(6): 774-80. doi: 10.1001/jamain-ternmed.2018.0743.
- Loggers S A I, Willems H C, van Balen R, Gosens T, Polinder S, Ponsen K J, et al. Evaluation of quality of life after nonoperative or operative management of proximal femoral fractures in frail institutionalized patients: the FRAIL-HIP study. JAMA Surg 2022; 157(5): 424-34. doi: 10.1001/jamasurg.2022.0089.