Radiographic signs and hip pain 5 years after THA with a cemented stem predict future revision for aseptic loosening: a prospective cohort study
Anne LÜBBEKE 1,2, Christophe BAREA 1, Matthieu ZINGG 1, Nicolas LAUPER 1, Didier HANNOUCHE 1, and Guido GARAVAGLIA 3
1 Division of Orthopaedics and Trauma Surgery, Geneva University Hospitals, University of Geneva, Faculty of Medicine, Geneva, Switzerland; 2 Nuffield Department of Orthopaedics, Rheumatology and Musculoskeletal Sciences, University of Oxford, Oxford, UK; 3 Ars Medica Centro Medico, Bellinzona, Switzerland
Background and purpose — We aimed to evaluate the long-term predictive value of radiographic abnormality and/or hip pain assessed 5 years following primary total hip arthroplasty (THA) and the occurrence of revision for aseptic loosening between 5 and 25 years postoperatively.
Patients and methods — We included all primary THAs performed between 1996 and 2011 (same uncemented cup, polyethylene-ceramic bearing, 28 mm head, cemented stem) and prospectively enrolled in the institutional registry, for whom baseline and follow-up radiographs were available. At 5 years radiographically we assessed femoral osteolysis and/or stem migration. Pain was evaluated with the Harris Hip pain subscore. Kaplan–Meier survival and Cox regression analyses were performed.
Results — 1,317 primary THAs were included. 25 THAs (2%) were revised for aseptic stem loosening. Any abnormal radiographic sign at 5 years was present in 191 THAs (14%). Occasional hip pain was reported by 20% and slight to severe pain by 12% of patients at 5 years. In patients < 60 years, 10 of the 12 later revised for aseptic stem loosening had abnormal radiographs at 5 years vs. 5 of the 13 later revised in those ≥ 60 years. Hazard ratios (HR) were 34 (95% confidence interval [CI] 7–155) in younger vs. 4 (CI 1–11) in the older group. HR for association of hip pain at 5 years with future revision was 3 (CI 1–5).
Conclusion — The presence of abnormal radiographic signs 5 years after THA was strongly associated with later revision for aseptic stem loosening, especially in patients < 60 years. The association between pain at 5 years and future revision was much weaker.
Citation: Acta Orthopaedica 2024; 95: 32–38. DOI: https://doi.org/10.2340/17453674.2023.26190.
Copyright: © 2024 The Author(s). This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (https://creativecommons.org/licenses/by-nc/4.0/), allowing third parties to copy and redistribute the material in any medium or format and to remix, transform, and build upon the material for non-commercial purposes, provided proper attribution to the original work.
Submitted: 2023-03-18. Accepted: 2023-11-02. Published: 2024-01-29.
Correspondence: anne.lubbekewolff@hcuge.ch
AL and GG designed the study, analyzed the data, and wrote the first draft of the manuscript. All authors contributed to data collection and manuscript reviewing.
The authors would like to thank all the patients, orthopedic surgeons, and the registry staff who have contributed to the Geneva Arthroplasty Registry since 1996. They would also like to thank Christophe Combescure (senior statistician) for most valuable help with the revision of the manuscript.
Handling co-editors: Marianne Westberg and Robin Christensen
Acta thanks Bart G Pijls and Stephan Maximilian Röhrl for help with peer review of this manuscript.
Aseptic loosening remains the main reason for long-term revision of a total hip arthroplasty (THA) [1-3]. A well-known risk factor for aseptic loosening and subsequent implant revision is age [4], which is closely related to the patient’s activity level [5]. The latter is considered one of the most influential factors for implant survival [6].
The introduction of a new implant should be done stepwise, to identify underperforming implants before they are implanted in a large number of people [7]—ideally without having to wait for the new implants’ 10–15-year revision rates. In this process clinically useful surrogate outcomes for revision that are measurable in the first years and reliably related to medium- to long-term failure are essential [8]. Surrogate outcomes for implant failure are sparse [9] but include imaging and clinical scores/patient-reported outcomes (PROs). It has been shown that continuous migration and early systematic radiographic analysis are useful in predicting midterm failure of both cemented and uncemented stems [10-12]. Moreover, few studies have examined the usefulness of PRO in predicting implant failure, and they focused on the short to midterm [13-15]. Thus, publications in this area consist of mostly smaller case series as imaging data and PROs/clinical scores are not always collected in national registries, and only a few institutional registries are systematically including them. The parameters may be used as surrogate measures for later failure.
We aimed to evaluate the predictive value of radiographic abnormality and/or hip pain development in the 5 years following primary THA by assessing the association between radiographic abnormalities and/or hip pain 5 years after surgery and the risk of stem revision for aseptic loosening up to 25 years after surgery among all and separately in young and older patients.
Patients and methods
Study population and study design
All patients undergoing THA since March 1996 were prospectively enrolled in a hospital-based registry. The institution is a large tertiary hospital and the only public hospital in the state/canton. For this study all patients undergoing primary elective THA between March 1996 and December 2011 with use of an uncemented monobloc cup, 28 mm head, ceramic-on-standard polyethylene bearing and a cemented stem were eligible. Completeness of recording of THAs is > 99% based on validation against the hospital’s diagnosis coding system; completeness of revision capture is > 96% based on data from the Swiss national joint registry (SIRIS). All patients in this cohort are systematically contacted for a clinical, radiological, and questionnaire follow-up visit with an orthopedic surgeon every 5 years. A telephone interview is scheduled in case the patient is unable or unwilling to attend the clinical visit.
Predictor, covariate, and outcome assessment
Information regarding baseline characteristics including age, sex, diagnosis, and surgical procedure was documented by the operating surgeon. Age at surgery was dichotomized (< 60 years vs. ≥ 60 years). The cut-off was chosen because—assuming a retirement age of 65 years—it includes the presumably most active working-age patients until the start of the analysis, which was 5 years after surgery. Moreover, a large population-based study [16] identified the cut-off of 60 years of age as most relevant in predicting future failure beyond the short term. Information concerning body mass index (BMI) and ASA score was retrieved from the anesthesia record. Information on death was obtained from the national death registry.
Outcome of interest was revision (stem only or total revision) for aseptic loosening. Information on revisions and their causes was obtained from the daily reporting of admissions to the orthopedic division for those revised at our institution and during the registry’s follow-up at 5-year intervals for those revised at another hospital. Detailed information regarding date, cause, and type of revision was extracted from the operative report and documented according to standardized categories. Hip pain was physician assessed at the 5-year clinical visit using the Harris Hip pain subscore, which has 6 response options rated from 0–44 (no pain). Assessment of radiological predictors is detailed in “Radiographic analysis.”
Implant- and technique-related information
For acetabular replacement the Morscher press-fit cup (Zimmer, Winterthur, Switzerland), an uncemented, nonmodular, Sulmesh-coated component was used. Very good mid- and long-term results have been reported for this cup [17]. The bearing surface was ceramic on ultra-high molecular weight polyethylene (UHMWPE). The stem was cemented (either Müller or Virtec stem, Sulzer Orthopedics, Baar, Switzerland) inserted via the lateral approach. Gentamycin-loaded bone cement was used, and cementing was performed using a third-generation technique with pulsed lavage and an intramedullary plug.
Radiographic analysis
Immediate and 5-year postoperative radiographs were analyzed by an experienced orthopedic surgeon blinded to the patients’ baseline characteristics and outcome. Evaluation was performed on digitized radiographs, and quantitative measurements were performed using specific templates and DICOMeasure software (ViewTec, Maison-Alfort, France). The diameter of the femoral head was used for calibration. Stem migration was measured from the tip of the greater trochanter to the shoulder of the prosthesis. Intra-rater reliability for the stem migration measurement based on 50 randomly selected radiographs measured at a 3-month interval using the intraclass correlation coefficient was 0.77 (95% confidence interval [CI] 0.63–0.87). Femoral osteolysis was defined as an area of endosteal, intracortical, or cancellous bone loss that was scalloped or had the appearance of bone destruction rather than osteopenia (Figure 1). We recorded the presence of focal osteolysis or radiolucent lines greater than 1 mm in width at the bone–cement interface, noting their dimension and location according to the zones of Gruen et al. Radiolucent lines of 2 mm or less in the proximal 1 cm of Gruen zones 1 and 7 on the anteroposterior view, and 8 and 14 on the lateral view were considered normal.

Figure 1. Radiographic example of osteolysis around the femoral stem.
Statistics
Occurrence of radiographic abnormalities and hip pain at 5 years were assessed overall and by age groups (< 60 and ≥ 60 years at surgery). Regarding associations, age (cut-off 60 years), presence or absence of the radiographic signs of stem migration and/or osteolysis, and presence or absence of hip pain 5 years after THA were evaluated, first separately and then combined, using Cox regression analysis with endpoint revision for aseptic loosening (either stem revision alone or total revision). Patients were followed up until revision for aseptic stem loosening, death, leaving the area of residency, or end of follow-up (August 31, 2022). Hazard ratios (HR) and 95% CIs were obtained for each predictor/predictor combination. To compare the predictive power of predictor combinations we calculated Harrell’s C-index (or concordance index) [18]. Finally, Kaplan–Meier failure curves were produced to illustrate differences in long-term outcome by predictor/predictor combination. Complete case analysis was conducted assuming that missing data on the predictors (radiographic abnormalities, hip pain) was missing completely at random. Covariates and outcome of patients eligible but with missing predictors were assessed to verify whether they were similar or not to those with available predictors.
Ethics, data sharing plan, funding, and disclosures
Ethics approval was obtained from the “Commission cantonale d’éthique de la recherche (CCER)” on October 11, 2022 (Project-ID 2022-00847). The manuscript was prepared according to the STROBE guidelines. The corresponding author can be contacted for data request. Institutional financial support for the registry was received from the “Fondation pour la recherche ostéo-articulaire.” All authors declare no conflicts of interests. Complete disclosure of interest forms according to ICMJE are available on the article page, doi: 10.2340/17453674.2023.26190
Results
Of the 2,401 THAs performed, 1,915 were eligible for the 5-year examination. Of those, 1,317 (69%) had complete radiographic follow-up including immediate postoperative and 5-year radiographs (Figure 2). Characteristics of the patients operated on and the characteristics of the patients still alive and eligible for examination at 5 years with complete vs. incomplete or absent radiographic information because of refusal to attend are given in Table 1. The starting point for the analysis was 5 years after surgery and patients were followed from there on average for 10 years (range 0.2–21), corresponding to 15 years since surgery (range 5–26). Overall, 29 revisions involving the stem were performed, 2 for prosthetic joint infection, 2 for periprosthetic facture, and 25 for aseptic stem loosening on average 13 years after surgery (range 5–19). Their mean age was 59 years, mean BMI 25, 64% were men. There were 12 revisions (9%) in the group < 60 years and 13 (1%) in the group ≥ 60 years. Radiographic analysis revealed stem migration ≥ 2 mm in 130 THAs (10%) at 5 years, linear/focal osteolysis in 67 THAs (5%), and any of these radiographic signs in 185 THAs (14%). Among those, 15 were later revised (8%), whereas among those with normal radiographs 10 (1%) were later revised. In 1,268 (97%) of the 1,317 THAs the HHS pain subscore at 5 years was recorded. No pain was reported for 866 THAs (68%), occasional pain for 255 THAs (20%), and slight to severe hip pain for 147 (12%).
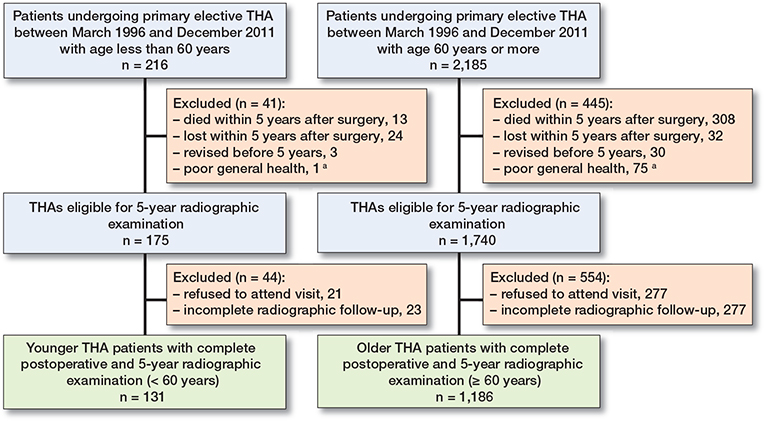
Figure 2. Flowchart of patient inclusions.a Poor general health (e.g., cancer, dementia) making it impossible to attend 5-year visit.
Occurrence of radiographic abnormalities and/or hip pain at 5 years by age groups
Abnormal radiographic signs at 5 years overall were present similarly frequently in the younger and older groups with 15% vs. 14%, respectively (Table 2). Hip pain of any degree at 5 years was reported by 43% of younger and by 30% of older patients. Younger patients reported significantly higher pain levels at 5 years. Among those with abnormal radiographic signs, hip pain (any) was slightly more frequent in the younger than in the older group with 50% (10 of 20 patients) vs. 35% (57 of 161), respectively.
| Age < 60 years | Age ≥ 60 years | Risk difference (CI) / P value a) | |
| Radiographic signs | 136 | 1,181 | |
| Stem migration ≥ 2mm | 17 (13) | 113 (9.6) | 2.9 (–2.9 to 8.7) |
| Linear/focal osteolysis | 7 (5.1) | 60 (5.1) | 0.0 (–3.9 to 4.0) |
| Any sign | 21 (15) | 164 (14) | 1.5 (–4.8 to 7.9) |
| Hip pain | 132 | 1,136 | P = 0.003 |
| None | 75 (57) | 791 (70) | |
| Occasional | 31 (24) | 224 (20) | |
| Mild | 11 (8.3) | 63 (5.5) | |
| Moderate | 10 (7.6) | 45 (4.0) | |
| Severe/extremely severe | 5 (3.8) | 13 (1.2) | |
| a P value obtained using Pearson chi-square test linear-by-linear association. | |||
Association of age, radiographic signs, and/or hip pain 5 years after surgery with future revision
Age at surgery, radiographic signs, and hip pain were evaluated first separately and then combined (Table 3). 48% of the patients revised were < 60 years at surgery compared with 10% of those unrevised (HR 6, CI 3–12). Presence of stem migration ≥ 2 mm or linear/focal osteolysis on 5-year radiographs significantly increased the risk of future revision for aseptic stem loosening (HR 9, CI 4–20) (Figure 3). Combining both signs compared with only 1 sign improved identification of future revisions (15/25 instead of 9–10/25) resulting in a greater Harrell’s C (0.8 vs. 0.7). Presence of any intensity of hip pain at 5 years was associated with an HR of 3 (CI 1–5) for future revision (Figure 4).
| Revised n = 25 | Not revised n = 1,292 | Hazard ratio (CI) a | Harrell’s C | |
| Age at surgery < 60 years | 12 (48) | 124 (9.6) | 5.6 (2.5–12.4) | 0.66 |
| Radiographic signs | ||||
| Stem migration ≥ 2 mm | 10 (40) | 120 (9.3) | 6.4 (2.9–14.2) | 0.70 |
| Linear/focal osteolysis | 9 (36) | 58 (4.5) | 9.7 (4.3–22.0) | 0.70 |
| Any sign | 15 (60) | 170 (13) | 8.9 (4.0–19.9) | 0.78 |
| Hip pain at 5 years | ||||
| Occasional to severe pain | 13 (52) | 389 (31) | 2.5 (1.1–5.4) | 0.60 |
| Age and radiographic signs | ||||
| Age < 60 years | 12 | 124 | ||
| No radiographic signs | 2 (17) | 113 (91) | Ref. | |
| Any radiographic signs | 10 (83) | 11 (8.9) | 34 (7.4–155) | 0.87 |
| Age ≥ 60 years | 13 | 1,168 | ||
| No radiographic signs | 8 (62) | 1,009 (86) | Ref. | |
| Any radiographic signs | 5 (38) | 159 (14) | 3.6 (1.2–11.2) | 0.69 |
| Age, pain, and radiographic signs b | ||||
| Age < 60 years | 12 | 120 | ||
| Pain no/yes, no radiographic signs c | 2 (17) | 110 (92) | Ref. | 0.89 |
| Pain no, any radiographic signs | 4 (33) | 6 (5.0) | 24 (4.4–132) | |
| Pain yes, any radiographic signs | 6 (50) | 4 (3.3) | 51 (10.1–252) | |
| Age ≥ 60 years b | 13 | 1,123 | ||
| Pain no, no radiographic signs | 6 (46) | 681 (61) | Ref. | 0. 69 |
| Pain yes, no radiographic signs | 2 (15) | 286 (26) | 0.9 (0.2–4.2) | |
| Pain no, any radiographic signs | 2 (15) | 102 (9.1) | 2.1 (0.4–10.4) | |
| Pain yes, any radiographic signs | 3 (23) | 54 (4.8) | 6.0 (1.5–25.1) | |
| a Hazard ratios (CIs) obtained using Cox regression. b 4 patients in the younger group had a missing value for hip pain and 45 in the older. c The 2 groups were combined because of 0 events in the “no pain, no radiographic signs” group. |
||||
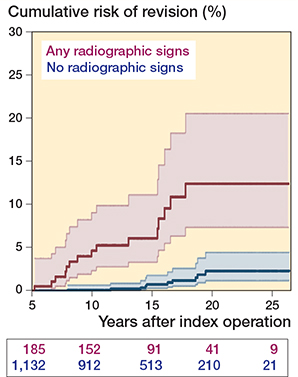
Figure 3. Cumulative risk of revision for aseptic stem loosening by presence or absence of radiographic signs at 5 years.
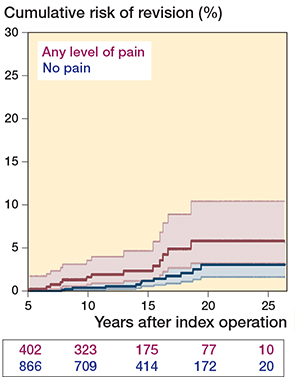
Figure 4. Cumulative risk of revision for aseptic stem loosening by presence or absence of hip pain at 5 years.
In the younger group, 10 of the 12 THAs later revised for aseptic stem loosening had abnormal radiographs 5 years after surgery compared with 5 of the 13 THAs later revised in the older group. Corresponding HRs were 34 (CI 7–155) vs. 4 (CI 1–11) and corresponding Harrell’s Cs were 0.9 vs. 0.7, respectively, indicating a substantially greater association of radiographic signs with later failure in younger patients (Table 3).
Cumulative incidences of failure 15 years after start of analysis (corresponding to 20 years postoperatively) were 2% (CI 1–5), 3% (CI 1–11), 4% (CI 2–9), and 53% (CI 32–76), respectively (Figure 5). Maintaining the stratification by age and adding the predictor pain to radiographic signs resulted in a marginally higher Harrell’s C of 0.9 in the younger and a similar one of 0.7 in the older (Table 3).
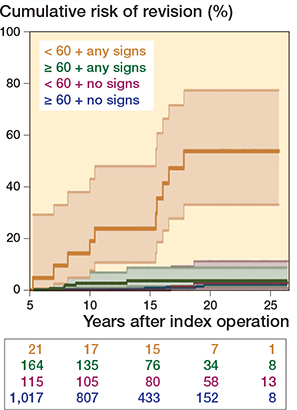
Figure 5. Cumulative risk of revision for aseptic stem loosening by age at surgery and presence or absence of radiographic signs at 5 years.
Discussion
This study assessed the usefulness of radiographic abnormalities including stem migration and osteolysis diagnosed on standard radiographs 5 years after surgery as well as the usefulness of pain assessment at 5 years to predict revision for aseptic stem loosening up to 25 years after THA. We found a strong association between radiographic abnormalities, symptomatic or not, and future revision in the younger patient group. The association was also present in the older group but was much less pronounced. The future risk of revision was more than 5 times higher in patients < 60 years compared with those ≥ 60 years. In the younger group, 83% of those later revised already had abnormal radiographs 5 years after surgery compared with 39% in the older group. The best performing predictor was presence of any radiographic signs—with stem migration and osteolysis individually performing equally well—followed by age at surgery. Hip pain at 5 years was the weakest predictor but still of value for predicting later revision. Younger patients presented more often with any degree of pain and slightly more often with pain and any radiographic signs 5 years after surgery than older patients.
Radiographic abnormalities as surrogate outcome of future revision
Within the follow-up of on average 14 years, 2% of the THAs were revised for aseptic stem loosening. In the literature, the long-term results of the implants used in this study (Morscher cup and Müller/Virtec stem) are documented as very good, and radiographic results and revision rates similar to ours have been reported [17,19].
The correlation between radiological signs and aseptic femoral loosening has also been shown for uncemented implants, and presence of radiolucencies, calcar remodeling, cortical thickening, pedestal, and subsidence have been associated with aseptic loosening [11,20,21]. For cemented implants radiological signs correlated to aseptic loosening are proximal osteopenia, cementing quality, subsidence, and radiolucencies, but most studies have explored only the signification of early femoral subsidence [22]. Only one previous publication by Kobayashi et al. [12] assessed the association between early radiographic signs including both migration and osteolysis on revision for aseptic stem loosening. They found a 27% risk for revision within the next 10 years in the presence of radiolucencies > 2 mm or femoral subsidence > 2 mm on the 2-year follow-up radiograph compared with 6% when radiographs were normal. The risk increased to 50% in the presence of both radiological signs. Our study confirms their findings in a large group of patients of young and old age. Moreover, we extended the follow-up period into the long term and demonstrate that early radiographic signs predict revision beyond the mid-term. The proportion of THAs revised for aseptic loosening was much lower though in our study despite the longer follow-up, which might relate to the improvement in survival since the 1980s and the younger age of their patients.
In contrast to previous publications, we evaluated the relation between radiographic abnormalities and revision in young and old patients. We found the association in both groups, but the magnitude was much greater in the younger group. One reason for this may be the difference in activity level, leading to quicker progression of radiographic signs and development of greater symptoms in the younger individuals. This was already visible at 5 years and has likely drifted further apart with longer usage between the young and old group, leading to more revisions in those who were younger. Another aspect is the decision to revise, which depends on the patient’s symptoms, activity level, and independence, and on surgery risk. The latter is linked to comorbidities and the complexity of the surgical intervention to be performed. Thus, in some instances older patients may have been less likely to be revised because of a higher risk and a lower expected benefit from the revision surgery. Among the patients with normal radiographs 5 years after surgery, representing the vast majority (90%) in this study, revision for aseptic loosening was rare; only 13 of the 1,182 (1.1%) were revised for aseptic stem loosening between 14 and 19 years after surgery. This questions the usefulness of routine radiographic follow-up beyond 5 years in patients with an established implant with good long-term results and with normal radiographs at 5 years.
Symptoms as surrogate outcome of future revision
Patients’ symptoms assessed either by the physician or self-reported have been studied regarding their usefulness as a predictor of future all-cause revision/reoperation after primary THA [13-15,23]. The reported follow-up times did not exceed 10 years. All studies found an increased risk of revision/reoperation with worsening scores using ratio measures in accordance with our results. Only Eneqvist et al. [14] calculated a concordance index, which was similar to ours (0.65 for VAS pain compared with 0.64 for hip pain in our study). In contrast to our study, none of the publications assessed both radiographic predictors and symptoms. Moreover, the low validity of clinical examination in the diagnosis of loosening of components compared with radiological assessment has been shown [24].
Limitations
This study includes only cemented stems. Due to the long-term follow-up highly crosslinked polyethylene was not evaluated, which may have changed the result. Only patients operated on via the lateral approach were included, which is why the results may not be valid for other approaches. Errors in subsidence measurement because of femur flexion with femoral stem magnification have been described [25], but when measuring subsidence as the distance from the greater trochanter to the shoulder of the prothesis, as we did here, the effect of femur tilt is reduced and is unlikely to influence the results. The extent of osteolysis was not assessed because of limited sample size. Other failure mechanisms such as wear, cup migration, proximal osteopenia, suboptimal cementing quality, and stem positioning were not evaluated, and they may perform differently as predictors. However, with migration and osteolysis we focused on the main predictors for femoral revision. Hip pain was evaluated using the surgeon-administered version of the HHS. Results might have differed slightly if a patient-reported version had been used [26].
Strengths
We included a homogeneous group of patients in terms of implants and surgical approach employed. Implants, type of fixation, and approach were commonly used at the time. We believe that the included patients are representative, as their characteristics only marginally differed for age and ASA score from those eligible for the 5-year examination but not included due to missing radiographic information or refusal. Moreover, the cumulative risk of revision for aseptic stem loosening was similar between the 2 groups (results not shown). The similarity of patient characteristics and outcomes does not suggest a risk of selection bias with the complete case analysis. However, the validity of the main analysis is based on the assumptions that predictors and outcome were missing completely at random [27].
Conclusions
Presence of stem migration or osteolysis and to a lesser degree presence of pain were associated with the risk of revision of cemented stems for aseptic loosening over the next 2 decades, especially in the young patient. This highlights the usefulness of early systematic radiographic assessment of cemented hip stems as part of the follow-up for both new and established implants. The performance of this or other types of imaging in predicting failure of hip prostheses made of newer materials demands further studies.
- Hopper R H Jr, Ho H, Sritulanondha S, Williams A C, Engh C A Jr. Otto Aufranc Award: Crosslinking reduces THA wear, osteolysis and revision rates at 15-year followup compared with noncrosslinked polyethylene. Clin Orthop Relat Res 2018; 476(2): 279-90. doi: 10.1016/j.arth.2023.01.028.
- Karachalios T, Komnos G, Koutalos A. Total hip arthroplasty: survival and modes of failure. EFORT Open Rev 2018; 3(5): 232-9. doi: 10.1302/2058-5241.3.170068.
- Feng X, Gu J, Zhou X. Primary total hip arthroplasty failure: aseptic loosening remains the most common cause of revision. Am J Transl Res 2022; 14(10): 7080–9.
- Prokopetz J J Z, Losina E, Bliss R L, Wright J, Baron J A, Katz J N. Risk factors for revision of primary total hip arthroplasty: a systematic review. BMC Musculoskelet Disord 2012; 13: 251. doi: 10.1186/1471-2474-13-251.
- Flugsrud G B, Nordsletten L, Espehaug B, Havelin L I, Meyer H E. The effect of middle-age body weight and physical activity on the risk of early revision hip arthroplasty: a cohort study of 1,535 individuals. Acta Orthop 2007; 78(1): 99-107. doi: 10.1080/17453670610013493.
- Schmalzried T P, Shepherd E F, Dorey F J, Jackson W O, dela Rosa M, Fa’vae F, et al. The John Charnley Award: wear is a function of use, not time. Clin Orthop 2000; 381: 36-46. doi: 10.1097/00003086-200012000-00005.
- Malchau H, Bragdon C R, Muratoglu O K. The stepwise introduction of innovation into orthopedic surgery: the next level of dilemmas. J Arthroplasty 2011; 26(6): 825-31. doi: 10.1016/j.arth.2010.08.007.
- Cipriano A, Ioannidis J P A, Rothwell P M, Glasziou P, Tianjing L, Hernandez A F, et al. Generating comparative evidence on new drugs and devices after approval. Lancet 2020; 395(10228): 998-1010. doi: 10.1016/S0140-6736(19)33177-0.
- Malak T T, Broomfield J A J, Palmer A J R, Hopewell S, Carr A, Brown C, et al. Surrogate markers of long-term outcome in primary total hip arthroplasty: a systematic review. Bone Joint Res 2016; 5: 206-14. doi: 10.1302/2046-3758.56.2000568.
- Krismer M, Biederman R, Stöckl B, Fischer M, Bauer R, Haid C. The prediction of failure of the stem in THR by measurement of early migration using EBRA-FCA. Einzel-Bild-Roentgen-Analyse-femoral component analysis. J Bone Joint Surg Br 1999; 81(2): 273-80. doi: 10.1302/0301-620x.81b2.8840.
- Streit M R, Haeussler D, Bruckner T, Proctor T, Innmann M M, Merle C, et al. Early migration predicts aseptic loosening of cementless femoral stems: a long-term study. Clin Orthop Relat Res 2016; 474: 1697-706. doi: 10.1007/s11999-016-4857-5.
- Kobayashi A, Donnelly W J, Scott G, Freeman M A. Early radiological observations may predict the long-term survival of femoral hip prostheses. J Bone Joint Surg Br 1997; 79(4): 583-9. doi: 10.1302/0301-620x.79b4.7210.
- Rothwell A G, Hooper G J, Hobbs A, Frampton C M. An analysis of the Oxford hip and knee scores and their relationship to early joint revision in the New Zealand Joint Registry. J Bone Joint Surg [Br] 2010; 92-B: 413-8. doi: 10.1302/0301-620X.92B3.22913.
- Eneqvist T, Nemes S, Bülow E, Mohaddes M, Rolfson O. Can patient-reported outcomes predict re-operations after total hip replacement? Int Orthop 2018; 42(2): 273-9. doi: 10.1007/s00264-017-3711-z.
- Devane P, Horne G, Gehling D. Oxford hip scores at 6 months and 5 years are associated with total hip revision within the subsequent 2 years. Clin Orthop Relat Res 2013; 471: 3870–4. doi: 10.1007/s11999-013-2880-3.
- Johnsen S P, Sørensen H T, Lucht U, Søballe K, Overgaard S, Pedersen A B. Patient-related predictors of implant failure after primary total hip replacement in the initial, short- and long-terms. J Bone Joint Surg Br 2006; 88(10): 1303-8. doi: 10.1302/0301-620X.88B10.17399.
- Gwynne-Jones D P, Lash H W R, James A W, Iosua E E, Matheson J A. The Morscher press-fit acetabular component: an independent long-term review at 18–22 years. J Arthroplasty 2017; 32(8): 2444-9. doi: 10.1016/j.arth.2017.02.052.
- Newson R B. Comparing the predictive powers of survival models. Stata J 2010; 10(3): 339-58. doi: 10.1177/1536867X1001000303.
- Clauss M, Bolliger L, Brandenberger D, Ochsner P E, Ilchmann T. Similar effect of stem geometry on radiological changes with 2 types of cemented straight stem. Acta Orthop 2016; 87(2): 120-5. doi: 10.3109/17453674.2015.1104153.
- Engh C A, Massin P, Suthers K E. Roentgenographic assessment of the biologic fixation of porous-surfaced femoral components. Clin Orthop Relat Res 1990; 257: 107-28.
- Garavaglia G, Gonzalez A, Barea C, Peter R, Hoffmeyer P, Lübbeke A, et al. Short stem total hip arthroplasty with the direct anterior approach demonstrates suboptimal fixation. Int Orthop 2021; 45(3): 575-83. doi: 10.1007/s00264-020-04910-5.
- van der Voort P, Bijls P G, Nieuwenhuijse M, Jasper J, Fiocco M, Plevier J W M, et al. Early subsidence of shape-closed hip arthroplasty stems is associated with late revision: a systematic review and meta-analysis of 24 RSA studies and 56 survival studies. Acta Orthop 2015; 86(5): 575-85. doi: 10.3109/17453674.2015.1043832.
- Singh J A, Schleck C, Harmsen S, Lewallen D. Clinically important improvement thresholds for Harris hip score and its ability to predict revision risk after primary total hip arthroplasty. BMC Musculoskelet Disord 2016; 17: 256. doi: 10.1186/s12891-016-1106-8.
- Roder C, Eggli S, Aebi M, Busato A. The validity of clinical examination in the diagnosis of loosening of components in total hip arthroplasty. J Bone Joint Surg Br 2003; 85(1): 37-44. doi: 10.1302/0301-620x.85b1.13367.
- Callary S A, Solomon L B, Holubowycz O T, Campbell D G, Howie D W. Accuracy of methods to measure femoral head penetration within metal-backed acetabular components. J Orthop Res 2017; 35(5): 988-96. doi: 10.1002/jor.23356.
- De Geofroy B, Ghabi A, Attas J, Micicoi L, Lopez M, de Dompsure R B, et al. Can hip function be assessed with self-report questionnaires? Feasibility study of a French self-report version of the Harris Hip and Merle d’Aubigné scores. Orthop Traumatol Surg Res 2023 Nov 1: 103746. doi: 10.1016/j.otsr.2023.103746.
- Christensen R, Ranstam J, Overgaard S, Wagner P. Guidelines for a structured manuscript: statistical methods and reporting in biomedical research journals. Acta Orthop 2023; 94: 243-9. doi: 10.2340/17453674.2023.11656.