6-month migration sufficient for evaluation of total knee replacements: a systematic review and meta-analysis
Raymond PUIJK 1, Rowan H PUIJK 1, Elise K LAENDE 2,3, Michael J DUNBAR 3,4, José W M PLEVIER 5, Peter A NOLTE 1,6, and Bart G C W PIJLS 7
1 Department of Orthopaedics, Spaarne Gasthuis, Hoofddorp, the Netherlands; 2 Mechanical and Materials Engineering, Queen’s University, Kingston, Ontario, Canada; 3 Division of Orthopaedics, Department of Surgery, Dalhousie University and QEII Health Sciences Centre, Nova Scotia Health Authority, Halifax, Nova Scotia, Canada; 4 School of Biomedical Engineering, Dalhousie University, Halifax, Nova Scotia, Canada; 5 Walaeus Library, Leiden University Medical Center, Leiden, The Netherlands; 6 Department of Oral Cell Biology, Academic Centre for Dentistry (ACTA), University of Amsterdam and Vrije Universiteit Amsterdam, Amsterdam, the Netherlands; 7 Department of Orthopaedics, Leiden University Medical Center, Leiden, The Netherlands.
Background and purpose — This updated meta-analysis evaluates the migration pattern of the tibial component of primary total knee replacements measured with radiostereometric analysis (RSA). We aimed to evaluate whether 6-month maximum total point motion (MTPM) values could be used instead of 1-year MTPM for RSA threshold testing and to present the pooled migration patterns for different implant designs that can be used as a benchmark.
Patients and methods — The search included all published RSA studies on migration patterns of tibial components until 2023. Study groups were classified according to their prosthesis brand, fixation, and insert (PFI). Sub-analyses were performed to compare the mean tibial component migration patterns of different implant variables, stratified according to fixation.
Results — 96 studies (43 new studies), including 197 study groups and 4,706 knees, were included. Most migration occurred within the first 6 postoperative months (126 study groups: mean 0.58 mm, 95% confidence interval [CI] 0.50–0.65), followed by minimal migration between 6 and 12 months (197 study groups: mean 0.04 mm, CI 0.03–0.06), irrespective of the fixation method used. Distinct migration patterns were observed among the different fixation methods. No differences were found in migration patterns among cemented components in any of the sub-group analyses conducted. For uncemented implants, trabecular metal surfaced components seemed to migrate less than porous-coated or uncoated components
Conclusion — Based on the small difference between MTPM values at 6 months and 1 year, MTPM at 6 months could be used instead of MTPM at 1 year for RSA threshold testing. The pooled migration patterns can be used as benchmark for evaluation of new implants by defining fixation-specific RSA thresholds when combined with implant survival.
Citation: Acta Orthopaedica 2023; 94: 577–587. DOI: https://doi.org/10.2340/17453674.2023.24579.
Copyright: © 2023 The Author(s). This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (https://creativecommons.org/licenses/by-nc/4.0/), allowing third parties to copy and redistribute the material in any medium or format and to remix, transform, and build upon the material for non-commercial purposes, provided proper attribution to the original work.
Submitted: 2023-04-22. Accepted: 2023-10-22. Published: 2023-11-30.
Correspondence: Rpuijk@spaarnegasthuis.nl
RP and BGP conceived the study. JWP designed the search strategy for the literature search. RP and RHP performed the study selection and data extraction. RP performed the analyses. RHP and BGP ensure the accuracy of data extraction. RP, EKL, MJD, PAN, and BGP helped with the interpretation of the results. RP wrote the manuscript.
The research group thanks the organization and audience of the 8th International RSA meeting in Nijmegen, the Netherlands, for awarding this study with the Edward Valstar award and for the pre-peer review of the study.
Handling co-editor: Li Felländer-Tsai,
Acta thanks Johan Kärrholm and Leif Ryd for help with peer review of this manuscript.
Over the last few decades, total knee arthroplasty has increased globally, mainly attributable to demographic factors such as an aging population, escalating obesity rates, and enhanced access to medical healthcare [1]. As a direct consequence of this trend, national arthroplasty registries have reported a similar increased incidence of revisions, with aseptic loosening as one of the predominant causes [2-4]. In an effort to reduce the need for revisions, total knee replacements (TKR) are continuously being developed, occasionally introducing less favorable designs [5]. Global regulation of new devices through regulatory guidelines is inconsistent, with many countries having underdeveloped regulations that lack premarket testing or rely solely on manufacturers proving substantial equivalence to a legally marketed implant. These regulations do not guarantee high-quality evidence to ensure the safety, reliability, and quality of new medical devices [6-8].
To address the potential introduction of unfavorable designs, standardization of joint replacement screening has been proposed and endorsed by multiple studies as a crucial part of the evaluation of new prostheses [9-18]. Radiostereometric analysis (RSA) studies have established implant migration benchmarks and thresholds in the early postoperative period to identify TKRs with increased migration as a surrogate measure for increased risk of aseptic loosening [10,12]. It would be beneficial if previously published thresholds based on 1-year migration could be moved to 6 months postoperatively, given the minimal increase in migration after 6 months [19]. However, in light of the continuous advancements in implant technology and the increasing number of RSA studies, it is imperative to evaluate this proposal. Therefore, we aimed primarily to compare the pooled 6-month and 1-year maximum total point motion (MTPM) values to explore the applicability of the 6-month MTPM values for future RSA threshold testing. Secondarily we aimed to describe migration patterns of the different design features stratified by fixation.
| All-poly | All-polyethylene |
| CI | Confidence Interval |
| CR | Cruciate retaining |
| CS | Condylar stabilized |
| FB | Fixed bearing |
| HA | Hydroxyapatite |
| HXLPE | Highly Crosslinked polyethylene |
| MB | Mobile bearing |
| MBRSA | Model-based RSA |
| MDR | Medical device regulation |
| MTPM | Maximum total point motion |
| PE | Polyethylene |
| PS | Posterior stabilized |
| RCT | Randomized controlled trial |
| RSA | Radiostereometric analysis |
| SD | Standard deviation |
| TKR | Total knee replacement |
| TM | Trabecular metal |
| UHMWPE | Ultra-high molecular weight polyethylene |
Material and methods
The reporting of this systematic review adheres to the standards of the updated Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA) Statement of 2020 [20]. This review serves as an update to the previous systematic review and meta-analysis published in 2018 [19]. The PRISMA checklist is itemized and available as Supplementary data on the article page.
This investigation was registered and embargoed in the Open Science Framework (OSF), a global study registry, accessible through the registration URL https://osf.io/96bnq/?view_only=0912275f5c364fffb3eec63921cf2925. During the study, there were protocol deviations, such as the decision not to use the software application “CADIMA” for screening purposes due to the time required for screening. As a result, Excel (version 16.69.1, Microsoft Corp, Redmond, WA, USA) was utilized for screening.
Eligibility criteria
Studies were eligible for inclusion if they investigated the migration patterns of the tibial component through RSA in patients who underwent primary TKR. Unpublished studies, protocols, databases, or manuscripts were also considered eligible. Studies were included if they examined: (1) primary tibial components; (2) migration patterns of at least 2 MTPM measurements by RSA during the first 2 postoperative years. All included studies from the initial review were included [19]. Non-clinical studies (e.g., animal, phantom) and articles written in languages other than English, Dutch, or German were excluded. Multiple studies with the same patient cohorts remained eligible if they reported additional follow-ups for migration pattern measurements.
Search strategy
The literature search from the previous systematic review and meta-analysis [19] (up to July 2016) was updated by a medical librarian (JP) to ensure comprehensive retrieval of all relevant studies. Multiple medical bibliographic databases were searched, including PubMed, Embase, Web of Science, the Cochrane Library, and Google Scholar. Each bibliographic database was consulted on May 5, 2022 and December 28, 2022. The search targeted studies published between January 1, 2016 (slight overlap with prior search) and December 28,2022. The search strategy employed combinations of controlled vocabulary and free text terms that were associated with: (1) RSA, and (2) total joint arthroplasty. No differentiation between knee and hip arthroplasty was made, as some studies report on both. The full search strategies for all databases including utilized filters are detailed in the Appendix.
Study selection
After combining the references from the individual databases, duplicates were removed by using the software application CADIMA [21]. Automatically removed duplicates were double-checked by the first reviewer (RP). The merged references were transferred to Excel for 2-stage screening, by 2 reviewers independently (RP, RHP). The screening was first based on the title and abstract, and, second, based on the full text. If the information in the abstract was insufficient or doubts existed, the study remained eligible for full-text screening. Any disagreement or uncertainty regarding study eligibility was resolved through consultation with a third reviewer (BP).
Data-collection process
Data from all newly included studies was collected by the first reviewer (RP) into an SPSS statistic database (version 27.0, IBM Corp, Armonk, NY, USA). No articles needed translation. Data from the initial meta-analysis was checked again by the first reviewer (RP), and the total database was independently checked by the second reviewer (RHP). Any missing or unclear information was obtained or confirmed by contacting the study investigators.
Data items
Data extracted from studies included migration in MTPM, and items regarding the study characteristics, patient demographics, RSA technique, and prosthesis characteristics. Details on extracted data items are presented in Table 1. In the case that a mean MTPM and corresponding SD were not reported, this was estimated from graphs by using the web application WebPlotDigitizer [22] or calculated from the reported median, interquartile range (IQR), or range by using an internationally accepted methodology [23]. MTPM data was considered at 6 weeks, 3 months, 6 months, 1 year, 2 years, 5 years, and 10 years postoperatively.
| Variable | Cemented | Uncemented | ||
| 6-months | 1-year | 6-months | 1-year | |
| Decades | ||||
| 1980s | 0.60 (0.32–0.88) | 0.71 (0.45–0.97) | 1.33 (1.03–1.64) | 1.27 (0.92–1.62) |
| 1990s | 0.50 (0.17–0.84) | 0.47 (0.37–0.58) | 1.55 (1.24–1.86) | 1.58 (1.26–1.89) |
| 2000s | 0.33 (0.25–0.41) | 0.39 (0.33–0.46) | 1.06 (0.57–1.54) | 0.91 (0.58–1.24) |
| 2010s | 0.38 (0.30–0.46) | 0.47 (0.39–0.55) | 0.85 (0.63–1.06) | 0.91 (0.70–1.12) |
| Surface modification | ||||
| Trabecular metal | n/a | n/a | 0.77 (0.56–0.98) | 0.74 (0.56–0.93) |
| Hydroxyapatite | n/a | n/a | 1.27 (0.71–1.83) | 1.15 (0.71–1.58) |
| Porous coating | n/a | n/a | 1.51 (1.22–1.79) | 1.46 (1.20–1.73) |
| Uncoated | n/a | n/a | 1.37 (1.07–1.68) | 1.43 (1.03–1.84) |
| Trabecular metal surfaced | ||||
| Modular | n/a | n/a | 0.84 (0.54–1.15) | 0.84 (0.57–1.12) |
| Non-modular | n/a | n/a | 0.70 (0.41–0.99) | 0.67 (0.42–0.92) |
| Tibial component design | ||||
| Metal backed | 0.37 (0.32–0.43) | 0.45 (0.40–0.50) | n/a | n/a |
| All-poly | 0.33 (0.12–0.53) | 0.38 (0.26–0.49) | n/a | n/a |
| Bearing mobility | ||||
| Fixed | 0.38 (0.32–0.44) | 0.44 (0.40–0.49) | 1.60 (1.26–1.93) a | 1.52 (1.23–1.82) a |
| Mobile | 0.36 (0.15–0.58) | 0.42 (0.20–0.63) | 1.22 (0.63–1.81) a | 1.24 (0.66–1.81) a |
| Insert constraint | ||||
| Cruciate retaining | 0.40 (0.30–0.51) | 0.45 (0.39–0.51) | 0.81 (0.51–1.10) b | 0.71 (0.51–0.91) b |
| Posterior stabilized | 0.43 (0.31–0.55) | 0.50 (0.40–0.61) | 0.72 (0.41–1.03) b | 0.90 (0.44–1.35) b |
| Condylar stabilized | 0.33 (0.22–0.44) | 0.39 (0.27–0.50) | n/a | n/a |
| Insert material | ||||
| UHMWPE | 0.38 (0.30–0.45) | 0.45 (0.40–0.51) | 0.73 (0.42–1.04) b | 0.67 (0.39–0.95) b |
| HXLPE | 0.34 (0.23–0.45) | 0.42 (0.34–0.51) | 0.81 (0.51–1.10) b | 0.82 (0.55–1.08) b |
| RSA technique | ||||
| Model-based RSA | 0.48 (0.35–0.60) | 0.56 (0.44–0.68) | 0.76 (0.30–1.22) b | 0.59 (0.38–0.80) b |
| Fictive point | 0.33 (0.24–0.42) | 0.39 (0.29–0.49) | 0.77 (0.49–1.05) b | 0.93 (0.59–1.26) b |
| Tibial baseplate marker | 0.39 (0.14–0.64) | 0.42 (0.27–0.57) | n/a | n/a |
| All-poly/n-mod marker | 0.36 (0.16–0.56) | 0.44 (0.32–0.56) | n/a | n/a |
| Modular PE marker | 0.38 (0.27–0.49) | 0.43 (0.36–0.51) | n/a | n/a |
| a Restricted to implants with a porous-coating surface. | ||||
| b Restricted to implants with a trabecular metal surface. | ||||
| MTPM, maximum total point motion; CI, confidence interval; UHMWPE, ultra high molecular weight polyethylene; HXLPE, highly crosslinked polyethylene; n-mod, non-modular; PE, polyethylene; n/a, not applicable. | ||||
Statistics
A study group was defined as a group of patients in a study with the same prosthesis, fixation, and insert (PFI), according to the PFI methodology used in previously published meta-analyses [10,19]. Pooling of migration results at the PFI level was performed using random effects meta-analyses by using the maximum-likelihood estimator [24]. The pooled mean MTPM and associated 95% confidence interval (CI) was calculated, presented, and compared between 6 months and 1 year after stratification for the 3 main fixation types (i.e., cemented vs. uncemented without screws vs. uncemented with screws). This also allowed the calculation of the mean difference between time points and their CI. Additionally, the 5th, 10th, 25th, 50th, 75th, 90th, and 95th percentiles and the pooled mean of the MTPM means were determined up to 5-year follow-up and plotted separately for both cemented and uncemented implants. As part of the sub-analyses, the pooled 1-year MTPM and CI was calculated and presented by PFI at each time point (i.e., 6 weeks, 3 months, 6 months, 1 year, 2 years, 5 years, and 10 years). The 1-year MTPM was used for these analyses, as this was the most frequently reported value, which reduces the risk of potential reporting bias or bias by missing data. Finally, study groups of studies were categorized based on the groups’ mean 1-year MTPM, according to the current RSA thresholds from 2012 [10] (1-year MTPM of < 0.5 mm [acceptable]; 0.5– 1.6mm [at risk]; > 1.6 mm [unacceptable]). To address potential issues with multicollinearity, several analyses of uncemented implants were stratified by surface modifications when these groups were highly correlated with certain covariates. All statistical analyses were conducted using R version 4.0.2 (R Foundation for Statistical Computing, Vienna, Austria) with the Metafor package (Maastricht University, Maastricht, Netherlands) [24].
Reporting bias assessment
The potential impact of publication bias and certainty of the results was evaluated by comparing the differences in MTPM values of certain implant characteristics (e.g., cruciate retaining [CR] and posterior stabilized [PS]) with the differences in revision rates for aseptic loosening of the same implant characteristics known from national registry reports.
Data sharing, funding, and disclosure
The data extraction of the RSA studies is available by contacting the corresponding author. Funding for the study was obtained from the author’s institution. BP and JP were authors of the previous systematic review and meta-analysis [19]. EL, MD, PN, and BP were part of an investigator team of multiple included studies. No author had any conflict of interest. Complete disclosure of interest forms according to ICMJE are available on the article page, doi: 10.2340/17453674.2023.24579
Results
Inclusion of RSA studies
The literature search yielded 2,319 records, of which 810 were duplicates. From the remaining 1,509 records, 1,404 were excluded for such reasons as not being a clinical study (n = 322), not involving primary TKRs (n = 678), or not including RSA measurements (n = 404). An additional 2 records were excluded because the full text was not retrievable. After reviewing 103 reports for eligibility, a total of 57 reports were excluded for the reasons stated in the PRISMA flow diagram (Figure 1). The remaining 46 reports, related to 43 original studies published since 1 January 2016, were included [25-70]. The previous review included 63 reports, related to 53 original studies published before 2016, with their reference stated in the previous paper [19]. The current review includes 109 reports related to 96 studies, comprising 197 study groups and 4,706 knees.
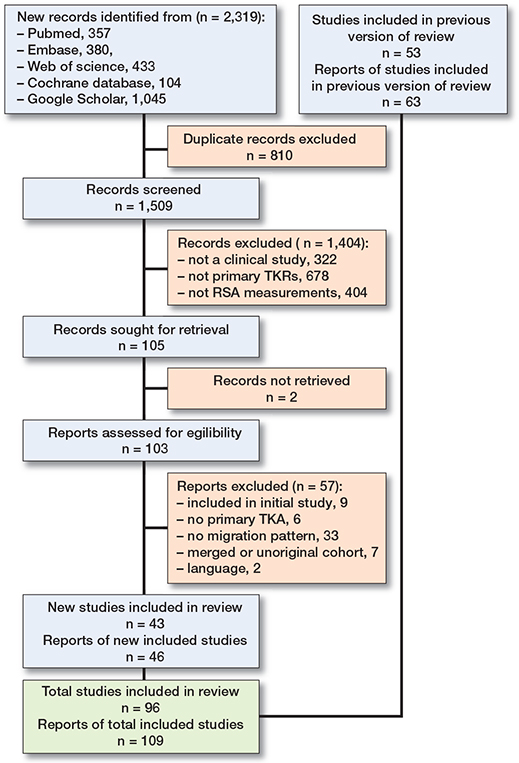
Figure 1. Flow diagram of articles screened, selected, and included in the systematic review and meta-analysis.
From each study group, the median percentage of females was 62% (medians ranging from 30–100%), the median age was 68 years (medians ranging from 54–77 years), and the median percentage of osteoarthritis was 100% (medians ranging from 0–100%). Tibial components were fixated with cement without screw-fixation in 128, cement with screw-fixation in 1, uncemented without screw-fixation in 51, and uncemented with screw-fixation in 17 study groups. An overall breakdown of the number of study groups and knees for the 3 main fixation types for each follow-up moment is detailed in Table 2.
The pooled mean MTPM of all tibial components was at 1 month 0.39 mm (CI 0.33–0.44, 3 months 0.44 mm (CI 0.40–0.49), 6 months 0.58 mm (CI 0.50–0.65), 1 year 0.55 mm (CI 0.50–0.60), 2 years 0.60 mm (CI 0.54–0.65), 5 years 0.68 mm (CI 0.57–0.80), and 10 years 0.72 mm (CI 0.49–0.96).
Migration patterns between 6-month and 1-year follow-up
For the overall group, the majority of the migration occurred within the first 6 months post-surgery of 0.58 mm (CI 0.50–0.65), whereafter minimal additional migration was observed between 6 months and 1 year of 0.04 mm (CI 0.03–0.06). Similarly, for the different fixation methods, most tibial component migration was observed within the first 6 months and changed between 6 months and 1 year by 0.04 mm (CI 0.02–0.06) for cemented, 0.05 mm (CI –0.03 to 0.13) for uncemented screw-fixated, and 0.06 mm (CI 0.01–0.11) for uncemented without screw-fixation. When cemented and uncemented components were stratified for different design factors, the majority of migration also occurred within the first 6 months for all comparisons (Table 1). Overall, the MTPM values were reported in 127 (64%) study groups at 6 months, compared with 197 (100%) study groups at 1-year follow-up (Table 2).
Migration patterns between fixation methods
The migration patterns of tibial components at 6 months showed that the pooled MTPMs were different between fixation groups: 0.37 mm (CI 0.31–0.42) for cemented, 0.67 mm (CI 0.47–0.86) for uncemented screw-fixated, and 1.13 mm (CI 0.96–1.31) for uncemented without screw-fixation (Figure 2). At 1-year follow-up, the differences in the pooled migration among all fixation methods remained: 0.43 mm (CI 0.38–0.47) for cemented, 0.77 mm (CI 0.56–0.98) for uncemented screw-fixated, and 1.08 mm (CI 0.9–1.24) for uncemented without screw-fixation. After 1 year, the slope of all 3 fixation methods changed, with a change between 1 and 5 years of 0.11 mm (CI 0.07–0.15) for cemented, 0.15 mm (CI 0.03–0.27) for uncemented screw-fixated, and 0.09 mm (CI –0.01 to 0.19) for uncemented without screw-fixation. The percentiles of the MTPM means were plotted separately up to a 5-year follow-up for cemented and uncemented without screw-fixation tibial components (Figure 3).
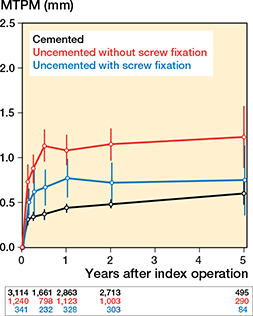
Figure 2. Migration patterns of all implants stratified by cemented, uncemented without screw fixation, and uncemented with screw fixation tibial components. The number of RSA examinations is given for each follow-up.
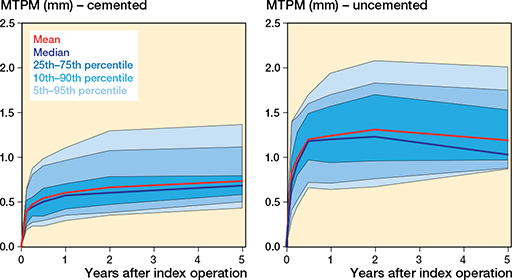
Figure 3. Early migration in percentiles of cemented (left) and uncemented (right) without screw-fixation tibial components.
Migration patterns within cemented tibial components
Migration patterns of cemented implants were lower in the last 3 decades than in the 1980s (Figure 4A). The migration of cemented metal-backed and all-poly implants seemed to be equal (Figure 4B). No variation in migration patterns seemed to exist between cemented implants with CR, PS, or CS inserts (Figure 4C), implants with UHMWPE or HXLPE insert material (Figure 4D), implants with fixed bearing (FB) or mobile bearing (MB) implants (Figure 4E), or when migration patterns were measured by different RSA and marker techniques (model-based RSA [MBRSA], marker-based RSA with fictive points, markers fixed to the tibial component, marker in all-poly or non-modular PE or markers in modular PE) (Figure 4F).
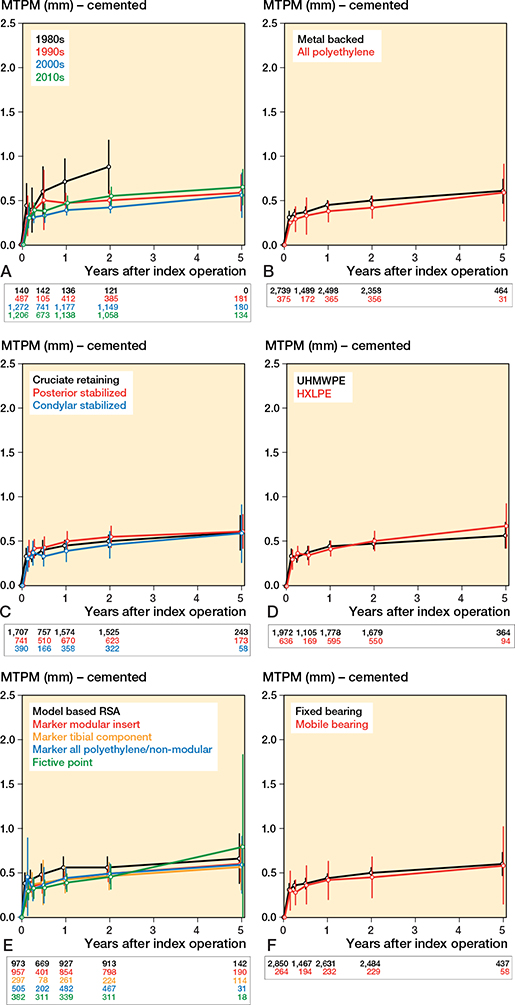
Figure 4. Migration patterns of cemented tibial components. The number of RSA examinations is given for each follow-up in color and order corresponding to the legend.
A. Migration patterns according to the decade in which the enrollment of the study started.
B. Migration patterns according to the design of the tibial baseplate.
C. Migration patterns according to the constraint of the insert.
D. Migration patterns according to the polyethylene material.
E. Migration pattern according to the mobility of the bearing.
F. Migration patterns according to the RSA technique used in the study.
Migration patterns within uncemented tibial components without screw fixation
Migration patterns of uncemented implants were substantially lower in the 2000s and 2010s than in the 1990s (Figure 5A). Only 2 study groups contained uncemented implants with an all-poly tibial baseplate design; all other implants had a metal-backed component, making a sub-analysis not applicable. A large variation in migration was found when components were categorized according to their surface modifications, with a substantially lower migration of trabecular-metal-(TM)-surfaced than porous-coated (sintered beads, plasma sprayed titanium) and uncoated components (waffled structure, fiber-mesh, grit-blasted, all-poly) (Figure 5B). Further analyses of design factors were limited to specific surface modifications on the tibial components due to the uneven distribution of these modifications. This restriction was applied when certain design factors were considered. After restriction to TM-surfaced tibial components, no variation in the migration earlier than 2 years seemed to exist between modular and non-modular implants (Table 1, Figure 5C), or between implants with UHMWPE and HXLPE inserts (Table 1, Figure 6A). The migration of TM-surfaced modular (Figure 5C) and HXLPE (Figure 6A) implants consists of the same study groups at 5 years with, as a result, the same increased migration between 2 and 5 years of 0.03 mm (CI –0.33 to 0.39). The same applies to TM-surfaced non-modular components (Figure 5C) and UHMWPE inserts (Figure 6A) at 5 years, with an equal migration between 2 and 5 years of 0.10 mm (CI –0.06 to 0.26). For CR and PS components (Figure 5D), or when measured with MBRSA and marker-based RSA with fictive points (Figure 6C), no variation in migration seemed to exist when restricted to TM-surfaced components. For bearing mobility, after restriction to porous-coated implants, no variation in migration was found between FB and MB implants (Figure 6B).
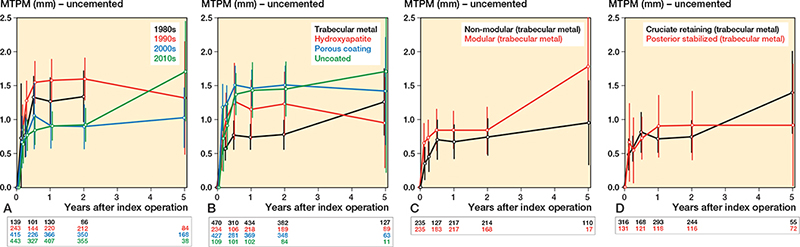
Figure 5. Migration patterns of uncemented without screw-fixation tibial components. The number of RSA examinations is given for each follow-up in color and order corresponding to the legend.
A. Migration patterns according to the decade in which the enrollment of the study started.
B. Migration patterns according to the components’ surface modification.
C. Migration pattern of modular and non-modular components, restricted to trabecular metal surfaced components.
D. Migration patterns according to the constraint of the insert, restricted to trabecular metal surfaced components.
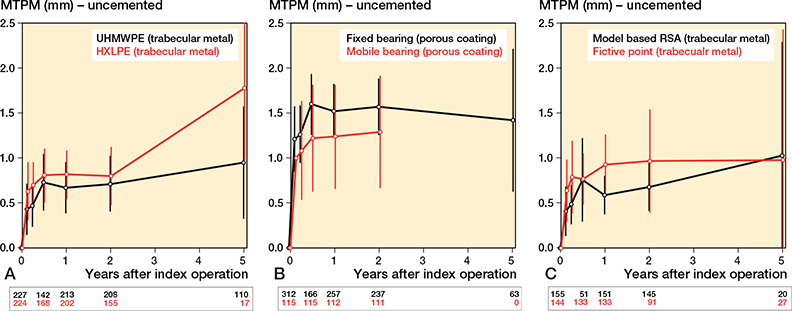
Figure 6. Migration patterns of uncemented without screw-fixation tibial components. The number of RSA examinations is given for each follow-up in color and order corresponding to the legend.
A. Migration patterns according to the polyethylene material, restricted to trabecular metal.
B. Migration patterns according to the mobility of the bearing, restricted to porous coating.
C. Migration patterns according to the RSA technique used, restricted to trabecular metal.
Classification of implant migration
The migration was “acceptable” in 47 (37%) cemented, 0 (0%) uncemented screw-fixated, and 1 (2%) uncemented without screw-fixation implant study groups, when these 197 study groups were categorized. An “at-risk” migration was found in 81 (63%) cemented, 15 (88%) uncemented screw-fixated, and 39 (76%) uncemented without screw-fixation implant study groups. An “unacceptable” migration was found in 0 (0%) cemented, 2 (12%) uncemented screw-fixated, and 11 (22%) uncemented without screw-fixation implant study groups. Of the 13 study groups with implants whose migration was classified as unacceptable, 9 of 13 (62%) study groups contained implants comprising older models, which are no longer used today. The distribution of categories (acceptable, at risk, unacceptable) was similar before and after 2012 (the year the classifications were defined) for both cemented and uncemented tibial components.
Discussion
Our study aimed to investigate the suitability of the 6-month MTPM values, as opposed to the conventional 1-year values, for RSA threshold testing. We showed that the implant migration primarily occurs during the initial 6 months postoperatively, followed by a stabilization phase (6–12 months) with minimal movement. Notably, this pattern holds true for all 3 fixation methods, even when considering more recent RSA studies that explore contemporary TKA designs.
As the migration from 6 months to 1 year is almost negligible, employing the 6-month MTPM values for RSA threshold testing reduces the time needed for RSA studies to be completed. This could potentially reduce attrition bias when patients are revised or lost to follow-up after 6 months. When 6-month MTPM is used for the thresholds, the time between 6 months and 12 months could be used to assess implant stabilization. The findings of this review highlight the importance of regularly evaluating data and benchmarks to keep up with the evolving landscape of orthopedic implants. The current RSA thresholds from 2012 [10] (< 0.5 mm [acceptable]; 0.5–1.6mm [at risk]; > 1.6 mm [unacceptable]) were based on the mean migration of a group of patients at 1 year. The thresholds were developed with patient safety in mind, as the absence of any phased evidence-based introduction was shown to be unsuccessful and detrimental to patients [5,17]. Consequently, despite the limited number of studies available at the time, it was necessary to establish reliable thresholds for an early version of a phased evidence-based introduction that would be strict enough to prevent potentially harmful implants from entering the market [17,71]. When considering the current migration threshold [10], most uncemented tibial components in this study were at more risk for late-term aseptic loosening than cemented implants. However, the equivalent stabilization after 6 months seems to suggest that they are equally well fixed, which is in line with the findings of the recent meta-analysis of Prasad et al. (2020), which found no difference in revision rates for aseptic loosening between fully cemented and uncemented TKR, after including 6 randomized controlled trials (RCT) with mid- to long-term follow-up [72].
For cemented implants, we found no substantial differences in migration patterns between all-poly and metalbacked tibial components; CR, PS, and CS implants; implants with UHMWPE and HXLPE inserts; FB and MB implants; or when measured by MBRSA or different marker-based RSA techniques. The results obtained in this study are in agreement with the outcomes found in our previous analysis [19] and suggest that comparable rates of revisions can be expected for aseptic loosening when assessing the impact of these variables through comparative research. These predictions are supported by the findings of systematic reviews and meta-analyses that include only RCTs with an extended follow-up period, which reported no difference in risk of revision for aseptic loosening between cemented all-poly and metal-backed TKR [73]; CR and PS TKR [74]; implants with UHMWPE and HXLPE inserts [75]; and between FB and MB implant designs [76].
For uncemented implants, our study showed a 0.28 mm increase in the 1-year pooled migration of HA-coated implants compared with the previous review [19]. This change was likely due to excluding a study group that used HA-coated implants but had an additional screw fixation. Furthermore, the distribution of the 1-year migration for TM-surfaced implants in the current study (0.74 mm; CI 0.56–0.93) was refined in contrast to that of the previous study (0.84 mm; CI 0.00–1.92) [19], which was attributed to the increasing number of studies investigating these implants. Additionally, we observed a substantial increase in the pooled continuous migration of modular TM implants from 2 to 5 years, compared with nonmodular TM implants (Figure 5C). The reason for this difference might be the greater flexibility of non-modular implants, where the PE insert is molded into the TM, which can improve load sharing and weight distribution on the tibial bone and reduce the chance of lift-off [52,77]. Overall, the favorable migration of TM components does align with the 0% aseptic loosening revision rates reported in a meta-analysis by Hu et al. (2017) of 307 non-modular TM implants after 5 years and a Finnish Registry study of 1,143 primary TKRs after 7 years [78,79]. On the other hand, our study does not reveal differences in migration based on the other sub-analyses of uncemented components (CR vs. PS; UHMWPE vs. HXLPE; FB vs. MB; MBRSA vs. marker-based RSA with fictive points), while registry data suggests higher rates of aseptic loosening of metal-backed than all-poly implants [80]; non-porous than porous-coated implants [81]; PS than CR cemented implants [82]; UHMWPE than HXLPE in cemented and uncemented implants [3,83] and MB than FB cemented and uncemented implants [84].
Limitations
First, the 6-month MTPM values were reported in only 64% of the study groups, which causes a higher number of missing values than at 1 year. This, in turn, leads to a reduction in RSA examinations and analytical precision, and the potential introduction of bias into the analysis. Second, wide CIs were observed, suggesting multicollinearity. Therefore, migration patterns should be considered as exploratory and not a formal comparison. To ensure the validity of the results, migration patterns were presented for each variable separately, stratified for the most influential independent variable (e.g., TM surface or porous coating) if necessary. Third, we did not account for translations and rotations when considering the migration in this study, while some authors have suggested it could also be used as a predictor of aseptic loosening [85]. However, inconsistent reporting of these parameters prompted us to focus on MTPM, a well-documented parameter for predicting loosening. Finally, because survival data was not incorporated into the study, no conclusions could be drawn regarding the suitability of the current migration thresholds. Combining rates with migration data is a massive undertaking that is beyond the scope of the present review. Therefore, we intend to update and re-evaluate the RSA thresholds using the migration data from this review.
Conclusion
This study demonstrates that the majority of implant migration occurs within the initial 6 months following arthroplasty, regardless of fixation method. These results advocate for employing the RSA threshold testing at 6 months, rather than at the traditional 1-year mark. By shortening this interval, potentially unsafe implants could be identified earlier, thereby protecting patients from unfavorable outcomes. Moreover, this study provided pooled migration patterns of different implant variables that can be used as a benchmark for future evaluation of new implants.
- Palazzo C, Nguyen C, Lefevre-Colau M M, Rannou F, Poiraudeau S. Risk factors and burden of osteoarthritis. Ann Phys Rehabil Med 2016; 59: 134-8. doi: 10.1016/J.REHAB.2016.01.006.
- Ben-Shlomo Y, Blom A, Boulton C, Brittain R, Clark E, Dawson-Bowling S, et al. National Joint Registry 19th Annual report 2022 (England, Wales, Northern Ireland, the Isle of Man and Guernsey) PMID: 36516281.
- Australian Orthopaedic Association National Joint Replacement Registry (AOANJRR). Hip, Knee & Shoulder Arthroplasty: 2022 Annual Report [Online]. https://aoanjrr.sahmri.com/documents/10180/732916/AOA+2022+AR+Digital/f63ed890-36d0-c4b3-2e0b-7b63e2071b16.
- NZOA Joint Registry/New Zealand Orthopaedic Association [Online]. [date unknown]. https://www.nzoa.org.nz/nzoa-joint-registry [March 3, 2023].
- Anand R, Graves S E, de Steiger R N, Davidson D C, Ryan P, Miller L N, et al. What is the benefit of introducing new hip and knee prostheses? J Bone Joint Surg Am 2011; 93(Suppl 3): 51-4. doi: 10.2106/JBJS.K.00867.
- Sorenson C, Drummond M. Improving medical device regulation: the United States and Europe in perspective. Milbank Q 2014; 92: 114. doi: 10.1111/1468-0009.12043.
- Hubner S, Maloney C, Phillips S D, Doshi P, Mugaga J, Ssekitoleko R T, et al. The evolving landscape of medical device regulation in East, Central, and Southern Africa. Glob Health Sci Pract 2021; 9: 136. doi: 10.9745/GHSP-D-20-00578.
- Gupta S K. Medical device regulations: a current perspective. J Young Pharmacists 2016; 8: 6-11. doi: 10.5530/JYP.2016.1.3.
- Malak T T, Broomfield J A J, Palmer A J R, Hopewell S, Carr A, Brown C, et al. Surrogate markers of long-term outcome in primary total hip arthroplasty: a systematic review. Bone Joint Res 2016; 5: 206-14. doi: 10.1302/2046-3758.56.2000568.
- Pijls B G, Valstar E R, Nouta K A, Plevier J W, Fiocco M, Middeldorp S, et al. Early migration of tibial components is associated with late revision: a systematic review and meta-analysis of 21,000 knee arthroplasties. Acta Orthop 2012; 83: 614-24. doi: 10.3109/17453674.2012.747052.
- Kärrholm J. Radiostereometric analysis of early implant migration: a valuable tool to ensure proper introduction of new implants. Acta Orthop 2012; 83: 551. doi: 10.3109/17453674.2012.745352.
- Ryd L, Albrektsson B E, Carlsson L, Dansgård F, Herberts P, Lindstrand A, et al. Roentgen stereophotogrammetric analysis as a predictor of mechanical loosening of knee prostheses. J Bone Joint Surg Br 1995; 77: 377-83.
- Pijls B G, Nieuwenhuijse M J, Schoones J W, Middeldorp S, Valstar E R, Nelissen R G H H. RSA prediction of high failure rate for the uncoated Interax TKA confirmed by meta-analysis. Acta Orthop 2012; 83: 142-7. doi: 10.3109/17453674.2012.672092.
- Hasan S, Mheen P J M de, Kaptein B L, Nelissen R G H H, Pijls B G. RSA-tested TKA implants on average have lower mean 10-year revision rates than non-RSA-tested sesigns. Clin Orthop Relat Res 2020; 478: 1232-41. doi: 10.1097/CORR.0000000000001209.
- Hasan S, Dijk L A van, Nelissen R G H H, Plevier J W M, Blankevoort L, Pijls B G. RSA migration of unicondylar knee arthroplasties is comparable to migration of total knee arthroplasties: a meta-analysis. J ISAKOS 7 (Elsevier) 2022; 17-23.
- van der Voort P, Pijls B G, Nieuwenhuijse M J, Jasper J, Fiocco M, Plevier J W, et al. Early subsidence of shape-closed hip arthroplasty stems is associated with late revision: a systematic review and meta-analysis of 24 RSA studies and 56 survival studies. Acta Orthop 2015; 86: 575-85. doi: 10.3109/17453674.2015.1043832.
- Nelissen R G H H, Pijls B G, Kärrholm J, Malchau H, Nieuwenhuijse M J, Valstar E R. RSA and registries: the quest for phased introduction of new implants. J Bone Joint Surg Am 2011; 93(Suppl. 3): 62-5. doi: 10.2106/JBJS.K.00907.
- Grewal R, Rimmer M G, Freeman M A R. Early migration of prostheses related to long-term survivorship: comparison of tibial components in knee replacement. J Bone Joint Surg- Series B 1992; 74: 239-42. doi: 10.1302/0301-620X.74B2.1544960.
- Pijls B G, Plevier J W M, Nelissen R G H H. RSA migration of total knee replacements: a systematic review and meta-analysis. Acta Orthop 2018; 89: 320-8. doi: 10.1080/17453674.2018.1443635.
- Page M J, McKenzie J E, Bossuyt P M, Boutron I, Hoffmann T C, Mulrow C D, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ 2021; 372: n71. doi: 10.1136/bmj.n71.
- Kohl C, McIntosh E J, Unger S, Haddaway N R, Kecke S, Schiemann J, et al. Online tools supporting the conduct and reporting of systematic reviews and systematic maps: a case study on CADIMA and review of existing tools. Environ Evid 2018; 7: 8. doi: 10.1186/s13750-018-0115-5.
- WebPlotDigitizer—Extract data from plots, images, and maps [Online]. https://automeris.io/WebPlotDigitizer/citation.html [February 15, 2023].
- Hozo S P, Djulbegovic B, Hozo I. Estimating the mean and variance from the median, range, and the size of a sample. BMC Med Res Methodol 2005; 5: 1-10. doi: 10.1186/1471-2288-5-13.
- Viechtbauer W. Conducting meta-analyses in R with the metafor package. J Stat Softw 2022; 36: 1-48. doi: 10.18637/jss.v036.i03.
- Teeter M G, Thoren J, Yuan X, McCalden R W, MacDonald S J, Lanting B A, et al. Migration of a cemented fixed-bearing, polished titanium tibial baseplate (genesis II) at ten years. Bone Joint J 2016; 98: 616-21. doi: 10.1302/0301-620X.98B5.36865.
- Broberg J S, Vasarhelyi E M, Lanting B A, Howard J L, Teeter M G. Migration and inducible displacement of the bicruciate-stabilized total knee arthroplasty: a randomized controlled trial of gap balancing and measured resection techniques. J Arthroplasty 2022; 37: 252-8. doi: 10.1016/j.arth.2021.10.010.
- Van Hamersveld K T, Marang-Van De Mheen P J, Nelissen R G H H R, Toksvig-Larsen S, Hamersveld K T van, Mheen P J M-V De, et al. Migration of all-polyethylene compared with metal-backed tibial components in cemented total knee arthroplasty. Acta Orthop 2018; 89: 412-17. doi: 10.1080/17453674.2018.1464317.
- van Ooij B, Sierevelt I N, van der Vis H M, Hoornenborg D, Haverkamp D. What is the role of cemented fixation in total knee arthroplasty? The two-year results of a randomized RSA controlled trial. Bone Joint J 2021; 103-b: 98-104. doi: 10.1302/0301-620x.103b1.bjj-2020-0788.r1.
- Winther N S, Jensen C L, Jensen C M, Lind T, Schrøder H M, Flivik G, et al. Comparison of a novel porous titanium construct (Regenerex) to a well proven porous coated tibial surface in cementless total knee arthroplasty: a prospective randomized RSA study with two-year follow-up. Knee 2016; 23: 1002-11. doi: 10.1016/j.knee.2016.09.010.
- Hasan S, Kaptein B L, Marang-van de Mheen P J, Van Hamersveld K T, Nelissen R G H H, Toksvig-Larsen S. Late stabilization after initial migration in patients undergoing cemented total knee arthroplasty: a 5-year follow-up of 2 randomized controlled trials using radiostereometric analysis. Acta Orthop 2022; 93: 271-6. doi: 10.2340/17453674.2022.1381.
- Koster L A, Rassir R, Kaptein B L, Sierevelt I N, Nelissen R G H H, Nolte P A. A randomized controlled trial comparing two-year postoperative femoral and tibial migration of a new and an established cementless rotating platform total knee arthroplasty. Bone Joint J 2023; 105-B: 148-57. doi: 10.1302/0301-620X.105B2.BJJ-2022-0414.R1.
- Wojtowicz R, Henricson A, Nilsson KG, Crnalic S. Uncemented monoblock trabecular metal posterior stabilized high-flex total knee arthroplasty: similar pattern of migration to the cruciate-retaining design—a prospective radiostereometric analysis (RSA) and clinical evaluation of 40 patients (49 knees). Acta Orthop 2019; 90: 460-6. doi: 10.1080/17453674.2019.1626097.
- Van Hamersveld K T, Marang-van de Mheen P J, Van Der Heide H J L, Van Der Linden-Van Der Zwaag H M J, Valstar E R, Nelissen R G H H. Migration and clinical outcome of mobile-bearing versus fixed-bearing single-radius total knee arthroplasty. Acta Orthop 2018; 89: 190-6. doi: 10.1080/17453674.2018.1429108.
- Van Hamersveld K T, Marang-Van De Mheen P J, Nelissen R, Toksvig-Larsen S. Peri-apatite coating decreases uncemented tibial component migration: long-term RSA results of a randomized controlled trial and limitations of short-term results. Acta Orthop 2018; 89: 425-30. doi: 10.1080/17453674.2018.1469223.
- van Hamersveld K T, Marang-van de Mheen P J, Tsonaka R, Valstar E R, Toksvig-Larsen S. Fixation and clinical outcome of uncemented periapatite-coated versus cemented total knee arthroplasty. Bone Joint J 2017; 99-B: 1467-76. doi: 10.1302/0301-620X.99B11.BJJ-2016-1347.R3.
- Øhrn F D, Leeuwen J Van, Tsukanaka M, Röhrl S. A 2-year RSA study of the Vanguard CR total knee system: a randomized controlled trial comparing patient-specific positioning guides with conventional technique. Acta Orthop 2018; 89: 418-24. doi: 10.1080/17453674.2018.1470866.
- Øhrn F D, Lian Ø B, Tsukanaka M, Röhrl S M. Early migration of a medially stabilized total knee arthroplasty: a radiostereometric analysis study up to two years. Bone Jt Open 2021; 2: 737-44. doi: 10.1302/2633-1462.29.BJO-2021-0115.R1.
- Teeter M G, Marsh J D, Howard J L, Vasarhelyi E M, McCalden R W, Naudie D D R, et al. A randomized controlled trial investigating the value of patient-specific instrumentation for total knee arthroplasty in the Canadian healthcare system. Bone Joint J 2019; 101: 565-72. doi: 10.1302/0301-620X.101B5.BJJ-2018-1323.R1.
- Stilling M, Mechlenburg I, Jepsen C F, Rømer L, Rahbek O, Søballe K, et al. Superior fixation and less periprosthetic stress-shielding of tibial components with a finned stem versus an I-beam block stem: a randomized RSA and DXA study with minimum 5 years follow-up. Acta Orthop 2019; 90: 165-71. doi: 10.1080/17453674.2019.1566510.
- Linde K N, Rytter S, Søballe K, Madsen F, Langdahl B, Stilling M. Component migration, bone mineral density changes, and bone turnover markers in cementless and cemented total knee arthroplasty: a prospective randomized RSA study in 53 patients with 2-year follow-up. Knee Surg Sports Traumatol Arthrosc 2022; 30(9): 3100-13. doi: 10.1007/s00167-022-06860-4.
- Ledin H, Good L, Johansson T, Aspenberg P. No effect of teriparatide on migration in total knee replacement. Acta Orthop 2017; 88: 259-62. doi: 10.1080/17453674.2017.1300745.
- Koster L A, Meinardi J E, Kaptein B L, Zwaag E V der L-Van der, Nelissen R G H H. Two-year RSA migration results of symmetrical and asymmetrical tibial components in total knee arthroplasty: a randomized controlled trial. Bone Joint J 2021; 103: 855-63. doi: 10.1302/0301-620X.103B5.BJJ-2020-1575.R2.
- Dunbar M J, Laende E K, Collopy D, Richardson C G. Stable migration of peri-apatite-coated uncemented tibial components in a multicentre study. Bone Joint J 2017; 99: 1596-1602. doi: 10.1302/0301620X.99B12.BJJ-2016-1118.R2.
- Laende E K, Wilson J L A, Flemming J M, Valstar E R, Richardson C G, Dunbar M J. Equivalent 2-year stabilization of uncemented tibial component migration despite higher early migration compared with cemented fixation: an RSA study on 360 total knee arthroplasties. Acta Orthop 2019; 90: 172-8. doi: 10.1080/17453674.2018.1562633.
- Ledin H, Good L, Aspenberg P. Denosumab reduces early migration in total knee replacement. Acta Orthop 2017; 88: 255-8. doi: 10.1080/17453674.2017.1300746.
- Christensson A, Tveit M, Kesteris U, Flivik G. Similar migration for medial congruent and cruciate-retaining tibial components in an anatomic TKA system: a randomized controlled trial of 60 patients followed with RSA for 2 years. Acta Orthop 2022; 93: 68-74. doi: 10.1080/17453674.2021.1983709.
- Schotanus M G M, Pilot P, Kaptein B L, Draijer W F, Tilman P B J, Vos R, et al. No difference in terms of radiostereometric analysis between fixed- and mobile-bearing total knee arthroplasty: a randomized, single-blind, controlled trial. Knee Surg Sports Traumatol Arthrosc 2017; 25: 2978-85. doi: 10.1007/s00167-016-4138-6.
- Molt M, Ryd L, Toksvig-Larsen S. A randomized RSA study concentrating especially on continuous migration. Acta Orthop 2016; 87: 262-7. doi: 10.3109/17453674.2016.1166876.
- Teeter M G, McCalden R W, Yuan X, MacDonald S J, Naudie D D. Predictive accuracy of RSA migration thresholds for cemented total hip arthroplasty stem designs. HIP Int 2018; 28: 363-8. doi: 10.1177/1120700018762179.
- Petursson G, Fenstad A M, Gøthesen Ø, Haugan K, Dyrhovden G S, Hallan G, et al. Similar migration in computer-assisted and conventional total knee arthroplasty. Acta Orthop 2017; 88: 166-72.
- Yilmaz M, Holm C, Lind T, Flivik G, Odgaard A, Petersen M. Bone remodeling and implant migration of uncemented femoral and cemented asymmetrical tibial components in total knee arthroplasty: a DEXA and RSA evaluation with 2-year follow-up. Knee Surg Relat Res 2021; 33: 25. doi: 10.1186/s43019-021-00111-5.
- Andersen M R, Winther N, Lind T, Schrøder H, Flivik G, Petersen M M. Monoblock versus modular polyethylene insert in uncemented total knee arthroplasty. Acta Orthop 2016; 87: 607-14. doi: 10.1080/17453674.2016.1233654.
- Henricson A, Nilsson K G. Trabecular metal tibial knee component still stable at 10 years. Acta Orthop 2016; 87: 504-10. doi: 10.1080/17453674.2016.1205169.
- Nivbrant N O, Khan R J K, Fick D P, Haebich S, Smith E. Cementless versus cemented tibial fixation in posterior stabilized total knee replacement: a randomized trial. J Bone Joint Surg Am 2020; 102: 1075-82. doi: 10.2106/JBJS.19.01010.
- Linde K N, Madsen F, Puhakka K B, Langdahl B L, Saballe K, Krog-Mikkelsen I, et al. Preoperative systemic bone quality does not affect tibial component migration in knee arthroplasty: a 2-year radiostereometric analysis of a hundred consecutive patients. J Arthroplasty 2019; 34: 2351-9. doi: 10.1016/j.arth.2019.05.019.
- Laende E K, Richardson C G, Meldrum A R, Dunbar M J. Tibial component migration after total knee arthroplasty with high-viscosity bone cement. J Arthroplasty 2021; 36: 2000-5. doi: 10.1016/j.arth.2021.01.081.
- Sporer S, MacLean L, Burger A, Moric M. Evaluation of a 3D-printed total knee arthroplasty using radiostereometric analysis: assessment of highly porous biological fixation of the tibial baseplate and metal-backed patellar component. Bone Joint J 2019; 101: 40-7. doi: 10.1302/0301-620X.101B7.BJJ-2018-1466.R1.
- Hasan S, Marang-Van De Mheen P, Kaptein B L, Nelissen R G H H, Toksvig-Larsen S. All-polyethylene versus metal-backed posterior stabilized total knee arthroplasty: similar 2-year results of a randomized radiostereometric analysis study. Acta Orthop 2019; 90: 590-5. doi: 10.1080/17453674.2019.1668602.
- Williams H A, Broberg J S, Howard J L, Lanting B A, Teeter M G. Effect of gap balancing and measured resection techniques on implant migration and contact kinematics of a cementless total knee arthroplasty. Knee 2021; 31: 86-96. doi: 10.1016/j.knee.2021.05.011.
- Torle J, Thillemann J K, Petersen E T, Madsen F, Søballe K, Stilling M. Less polyethylene wear in monobloc compared to modular ultra-high-molecular-weight-polyethylene inlays in hybrid total knee arthroplasty: a 5-year randomized radiostereometry study. Knee 2021; 29: 486-99. doi: 10.1016/j.knee.2021.02.033.
- Laende E K, Richardson C G, Dunbar M J. A randomized controlled trial of tibial component migration with kinematic alignment using patient-specific instrumentation versus mechanical alignment using computer-assisted surgery in total knee arthroplasty. Bone Joint J 2019; 101: 929-40. doi: 10.1302/0301-620X.101B8.BJJ-2018-0755.R3.
- Teeter M G, Perry K I, Yuan X, Howard J L, Lanting B A. Contact kinematics correlates to tibial component migration following single radius posterior stabilized knee replacement. J Arthroplasty 2018; 33: 740-5. doi: 10.1016/j.arth.2017.09.064.
- Mosegaard B S, Rytter S, Madsen F, Odgaard A, Søballe K, Stilling M. Two-year fixation and ten-year clinical outcomes of total knee arthroplasty inserted with normal-curing bone cement and slow-curing bone cement: a randomized controlled trial in 54 patients. Knee 2021; 33: 110-24. doi: 10.1016/j.knee.2021.08.027.
- Laende E K, Flemming J M, Astephen Wilson J L, Cantoni E, Dunbar M J. The associations of implant and patient factors with migration of the tibial component differ by sex: a radiostereometric study on more than 400 total knee arthroplasties. Bone Joint J 2022; 104-B(4): 444-51.doi: 10.1302/0301-620X.104B4.BJJ-2021-1247.R1.
- Dyreborg K, Winther N, Lind T, Flivik G, Petersen M. Evaluation of different coatings of the tibial tray in uncemented total knee arthroplasty: a randomized controlled trial with 5 years follow-up with RSA and DEXA. Knee 2021; 29: 208-15. doi: 10.1016/j.knee.2021.02.002.
- Hasan S, Hamersveld K T V, Van de Mheen P J M, Kaptein B L, Nelissen R G H H, Toksvig-Larsen S. Migration of a novel 3D-printed cementless versus a cemented total knee arthroplasty: two-year results of a randomized controlled trial using radiostereometric analysis. Bone Joint J 2020; 102: 1016-24. doi: 10.1302/0301-620X.102B8.BJJ-2020-0054.R1.
- Kaptein B L, Hollander P den, Thomassen B, Fiocco M, Nelissen R G H H. A randomized controlled trial comparing tibial migration of the ATTUNE cemented cruciate-retaining knee prosthesis with the PFC-sigma design. Bone Joint J 2020; 102: 1158-66. doi: 10.1302/0301-620X.102B9.BJJ-2020-0096.R1.
- Laende E K, Dunbar M J, Richardson C G. Predictive value of short-term migration in determining long-term stable fixation in cemented and cementless total knee arthroplasties. Bone Joint J 2019; 101: 55-60. doi: 10.1302/0301-620X.101B7.BJJ-2018-1493.R1.
- Troelsen A, Ingelsrud L H, Thomsen M G, Muharemovic O, Otte K S, Husted H. Are there differences in micromotion on radiostereometric analysis between bicruciate and cruciate-retaining designs in TKA? A randomized controlled trial. Clin Orthop Relat Res 2020; 478: 2045-53. doi: 10.1097/CORR.0000000000001077.
- Mills K, Wymenga A B, Bénard M R, Kaptein B L, Defoort K C, van Hellemondt G G, et al. Fluoroscopic and radiostereometric analysis of a bicruciate-retaining versus a posterior cruciate-retaining total knee arthroplasty: a randomized controlled trial. Bone Joint J 2023; 105-B: 35-46. doi: 10.1302/0301-620X.105B1.BJJ-2022-0465.R2.
- Pijls B G, Nelissen R G H H. The era of phased introduction of new implants. Bone Joint Res 2016; 5: 215-17. doi: 10.1302/2046-3758.56.2000653.
- Prasad A K, Tan J H S, Hanna S A, Dawson-Bowling S, Bedair H S. Cemented vs. cementless fixation in primary total knee arthroplasty: a systematic review and meta-analysis. EFORT Open Rev 2020; 5: 793-8. doi: 10.1302/2058-5241.5.200030.
- Nouta K A, Verra W C, Pijls B G, Schoones J W, Nelissen R G H H. All-polyethylene tibial components are equal to metal-backed components: systematic review and meta-regression. Clin Orthop Relat Res 2012; 470: 3549-59. doi: 10.1007/s11999-012-2582-2.
- Jiang C, Liu Z, Wang Y, Bian Y, Feng B, Weng X. Posterior cruciate ligament retention versus posterior stabilization for total knee arthroplasty: a meta-analysis. PLoS One 2016; 11: e0147865, doi: 10.1371/JOURNAL.PONE.0147865.
- Bistolfi A, Giustra F, Bosco F, Faccenda C, Viotto M, Sabatini L, et al. Comparable results between crosslinked polyethylene and conventional ultra-high molecular weight polyethylene implanted in total knee arthroplasty: systematic review and meta-analysis of randomised clinical trials. Knee Surg Sports Traumatol Arthrosc 2022; 30: 3120-30. doi: 10.1007/s00167-022-06879-7.
- Hofstede S N, Nouta K A, Jacobs W, van Hooff M L, Wymenga A B, Pijls B G, et al. Mobile bearing vs fixed bearing prostheses for posterior cruciate retaining total knee arthroplasty for postoperative functional status in patients with osteoarthritis and rheumatoid arthritis. Cochrane Database Syst Rev 2015; (2): CD003130. doi: 10.1002/14651858.CD003130.PUB3.
- Dunbar M J, Wilson D A, Hennigar A W, Amirault J D, Gross M, Reardon G P, et al. Fixation of a trabecular metal knee arthroplasty component: a prospective randomized study. J Bone Joint Surg Am 2009; 91: 1578-86. doi: 10.2106/jbjs.h.00282.
- Hu B, Chen Y, Zhu H, Wu H, Yan S. Cementless porous tantalum monoblock tibia vs cemented modular tibia in primary total knee arthroplasty: a meta-analysis. J Arthroplasty 2017; 32: 666-74. doi: 10.1016/j.arth.2016.09.011.
- Niemeläinen M, Skyttä E T, Remes V, Mäkelä K, Eskelinen A. Total knee arthroplasty with an uncemented trabecular metal tibial component: a registry-based analysis. J Arthroplasty 2014; 29: 57-60. doi: 10.1016/J.ARTH.2013.04.014.
- Gudnason A, Hailer N P, W-Dahl A, Sundberg M, Robertsson O. All-polyethylene versus metal-backed tibial components: an analysis of 27,733 cruciate-retaining total knee replacements from the Swedish knee arthroplasty register. J Bone Joint Surg 2014; 96: 994-9. doi: 10.2106/JBJS.M.00373.
- Puijk R, Rassir R, Sierevelt I N, Spekenbrink-Spooren A, Nelissen R G H H, Nolte P A. Association between surface modifications for biologic fixation and aseptic loosening of uncemented total knee arthroplastiess. J Arthroplasty 2023; S0883-5403(23)00634-4. doi: 10.1016/j.arth.2023.05.094.
- Spekenbrink-Spooren A, Van Steenbergen L N, Denissen G A W, Swierstra B A, Poolman R W, Nelissen R G H H. Higher mid-term revision rates of posterior stabilized compared with cruciate retaining total knee arthroplasties: 133,841 cemented arthroplasties for osteoarthritis in the Netherlands in 2007-2016. Acta Orthop 2018; 89: 640-5. doi: 10.1080/17453674.2018.1518570.
- LROI. LROI Annual Report 2022. Information on orthopaedic prosthesis procedures in the Netherlands [Online]. https://www.lroi-report.nl/ [February 23, 2023].
- Gothesen O, Lygre S H L, Lorimer M, Graves S, Furnes O. Increased risk of aseptic loosening for 43,525 rotating-platform vs. fixed-bearing total knee replacements: a Norwegian-Australian registry study, 2003–2014. Acta Orthop 2017; 88: 649. doi: 10.1080/17453674.2017.1378533.
- Gudnason A, Adalberth G, Nilsson K G, Hailer N P. Tibial component rotation around the transverse axis measured by radiostereometry predicts aseptic loosening better than maximal total point motion: a follow-up of 116 total knee arthroplasties after at least 15 years. Acta Orthop 2017; 88: 282-7. doi: 10.1080/17453674.2017.1297001.
Appendix
Details of the literature search strategy
| PubMed ((“Photogrammetry”[ Mesh:NoExp] OR Radiostereometric Analysis [Mesh] OR “roentgen stereophotogrammetric analysis”[tiab] OR “RSA” [tiab] OR “Radiostereometric” [tiab] OR “Radiostereometrics” [tiab] OR “stereophotogrammetric” [tiab] OR “stereophotogrammetrics” [tiab] OR “stereophotogrammetry” [tiab] OR “stereo-photogrammetric” [tiab] OR “stereophotogrammetrics” [tiab] OR “stereophotogrammetry” [tiab] OR “Photofluorography” [Mesh] OR “roentgen fluoroscopic”[tiab] OR “roentgen fluoroscopics”[tiab] OR “roentgen fluoroscopy”[tiab])) AND ((“Joint Prosthesis”[Mesh:NoExp] OR “Hip Prosthesis”[Mesh] OR “Knee Prosthesis”[Mesh] OR “hip prosthesis”[tiab] OR “knee prosthesis”[tiab] OR “hip prostheses”[tiab] OR “knee prostheses”[tiab] OR “prosthetic hip”[tiab] OR “prosthetic knee”[tiab] OR “TKA”[tiab] OR “THA”[tiab] OR “THR”[tiab] OR “TKR”[tiab] OR “joint replacement”[tiab] OR “Arthroplasty, Replacement”[mesh:NoExp] OR “total knee replacement”[tiab] OR “total hip replacement”[tiab] OR “total knee arthroplasty”[tiab] OR “total hip arthroplasty”[tiab] OR “Arthroplasty, Replacement, Hip”[Mesh] OR “Arthroplasty, Replacement, Knee”[Mesh])) AND (“2016”[Date - Publication] : “2023”[Date - Publication]) |
| Web of Science TS=(“Photogrammetr*” OR “RSA” OR “radiostereometr*” OR “radio-stereometr*” OR “stereophotogrammetr*” OR “stereo-photogrammetr*” OR “roentgen fluoroscop*” OR “Photofluorograph*” OR “Photo-fluorograph*”) AND TS=(“Joint Prosthe*” OR “hip prosthe*” OR “knee prosthe*” OR TKA OR TKR OR THA OR THR OR “hip arthroplast*” OR “knee arthroplast*” OR “knee replacement*” OR “hip replacement*”) AND PY=(2016-2023) |
| Cochrane database (“Photogrammetr*” OR “RSA” OR “radiostereometr*” OR “radio-stereometr*” OR “stereophotogrammetr*” OR “stereo-photogrammetr*” OR “roentgen fluoroscop*” OR “Photofluorograph*” OR “Photofluorograph*”):ti,ab,kw AND (“Joint Prosthe*” OR “hip prosthe*” OR “knee prosthe*” OR TKA OR TKR OR THA OR THR OR “hip arthroplast*” OR “knee arthroplast*” OR “knee replacement*” OR “hip replacement*”):ti,ab,kw |
| Embase (Stereophotogrammetry/ OR exp radiostereometric analysis/ OR “RSA”.ti,ab. OR “Radiostereometr*”. ti,ab. OR “Radio-stereometr*”.ti,ab. OR “stereophotogrammetr*”.ti,ab. OR “stereo-photogrammetr*”. ti,ab. OR exp fluorography/ OR “Photofluorograph*”.ti,ab. OR “Photo-fluorograph*”.ti,ab. OR “roentgen fluoroscop*”.ti,ab.) AND (joint prosthesis/ OR exp hip prosthesis/ OR exp knee prosthesis/ OR “hip prosthe*”.ti,ab. OR “hip arthroplast*”.ti,ab. OR “hip replacement*”.ti,ab. OR “knee prosthe*”.ti,ab. OR “knee arthroplast*”.ti,ab. OR “knee replacement*”.ti,ab. OR “prosthetic hip*”.ti,ab. OR “prosthetic knee*”. ti,ab. OR “TKA”.ti,ab. OR “TKR”.ti,ab. OR “THA”.ti,ab. OR “THR”.ti,ab. OR “joint replacement*”.ti,ab. OR replacement arthroplasty/ OR exp hip replacement/ OR exp knee replacement/) AND 2016:2023. (sa_year). NOT (conference OR conference abstract OR “conference review”).pt. |
| Google Scholar “Total knee arthroplasty” AND “radiostereometric” from 2016 to 2023, no citations, no patents |