Radiographic reference values of the central knee anatomy in 8–16-year-old children
Bjoern VOGT 1,a, Emma HVIDBERG 2,3,a, Jan Duedal RÖLFING 1-3, Georg GOSHEGER 4, Bjarne MØLLER-MADSEN 2,3, Ahmed A ABOOD 2,3, Veronika WEYER-ELBERICH 5, Andrea LAUFER 1,4, Gregor TOPOROWSKI 1,4, Robert ROEDL 1, and Adrien FROMMER 1,4
1 Pediatric Orthopedics, Deformity Reconstruction and Foot Surgery, Muenster University Hospital, Germany; 2 Danish Pediatric Orthopedic Research, Aarhus University Hospital, Denmark; 3 Children’s Orthopaedics and Reconstruction, Aarhus University Hospital, Denmark; 4 General Orthopedics and Tumor Orthopedics, Muenster University Hospital, Germany; 5 Institute of Biostatistics and Clinical Research, University of Muenster, Germany
a Shared first authorship
Background and purpose — For correction of leg-length discrepancy or angular deformity of the lower limb in skeletally immature patients temporary or permanent (hemi-)epiphysiodesis can be employed. These are reliable treatments with few complications. Recently, radiographic analysis of treatment-related alterations of the central knee anatomy gained interest among pediatric orthopedic surgeons. To date the comparison and adequate interpretation of potential changes of the central knee anatomy is limited due to the lack of defined standardized radiographic references. We aimed to establish new reference values of the central knee anatomy.
Patients and methods — A retrospective analysis of calibrated longstanding anteroposterior radiographs of 254 skeletally immature patients with a chronological age ranging from 8 to 16 years was conducted. The following radiographic parameters were assessed: (1) femoral floor angle, (2) tibial roof angle, (3) width at femoral physis, and (4) femoral notch–intercondylar distance.
Results — All observed radiographic parameters were normally distributed with a mean age of 12.4 years (standard deviation [SD] 2, 95% confidence interval [CI] 12.2–12.6). Mean femoral floor angle was 142° (SD 6, CI 141.8–142.9), mean tibial roof angle was 144° (SD 5, CI 143.7–144.1), mean width at femoral physis was 73 mm (SD 6, CI 72.8–73.9), and mean femoral notch–intercondylar distance was 8 mm (SD 1, CI 7.5–7.7). The estimated intraclass correlation coefficient values were excellent for all measurements.
Conclusion — This study provides new radiographic reference values of the central knee anatomy for children between 8 and 16 years and we suggest considering values within the range of 2 SD as the physiological range.
Citation: Acta Orthopaedica 2023; 94: 393–398. DOI: https://doi.org/10.2340/17453674.2023.15336.
Copyright: © 2023 The Author(s). This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (https://creativecommons.org/licenses/by-nc/4.0/), allowing third parties to copy and redistribute the material in any medium or format and to remix, transform, and build upon the material for non-commercial purposes, provided proper attribution to the original work.
Submitted: 2023-04-01. Accepted: 2023-06-08. Published: 2023-07-31.
Correspondence: bjoern.vogt@ukmuenster.de
Study design, conceptulization, methods: all authors; resources: GG, BMM, RR; supervision: JDR, GG; BMM, AAA, RR, AF; data collection: EH, BV, JDR, AL, GT, AF; data analysis: VWE, BV, EH, JDR, AF; interpretation of results: all authors; writing the first draft: EH, BV, JDR, AF; critical revision: GG, BMM, AAA, VWE, AL, GT, RR; final approval: all authors; revision after peer-review: JDR, EH, BV, AF.
Handling co-editors Ilkka Helenius
Acta thanks Franck Accadbled, Andreas Krieg, and Jaap Tolk for help with peer review of this manuscript.
In growing patients, (hemi-)epiphysiodesis of the distal femur and proximal tibia is an established treatment to correct leg length discrepancies (LLD) and angular lower limb deformities [1-6]. For correction of LLD, permanent or temporary operation techniques are commonly employed [1,2,7-9]. For gradual correction of angular deformities of the lower limb in skeletally immature patients, temporary hemi-epiphysiodesis is the preferred surgical treatment [4-6,10]. Several previous studies have shown that epiphysiodesis is a reliable approach with few complications [1,4,6,11,12].
However, there is a lack of studies that have reliably assessed the influence of epiphysiodesis on the knee joint in the coronal plane or the central knee anatomy. As regards the central intra-articular anatomy of the knee, recent studies have tried to investigate the effects of epiphysiodesis [13-15]. However, sample sizes are relatively small with heterogeneous patient cohorts and there is a lack of standardized radiographic reference values that help to differentiate physiological from pathological limb alignment and knee joint configuration in growing patients.
Detailed knowledge of physiological limb alignment and knee joint configuration is helpful for adequate treatment of limb deformities and LLD. The established joint orientation angles described by Paley and the mechanical axis deviation (MAD) described by Moreland et al. have improved the field of pediatric orthopedics and limb reconstruction [16,17]. Regarding epiphysiodesis, just recently a new radiographic reference for the height of the proximal fibula in children was described to assess the necessity of concomitant proximal fibular epiphysiodesis during correction of LLD by growth arrest through epiphysiodesis around the knee [18]. This indicates that radiographic references are helpful to assess treatment-related alteration of knee joint anatomy in skeletally immature patients treated by epiphysiodesis. We analyzed 4 specific radiographic parameters of coronal central knee anatomy in healthy knees of skeletally immature individuals. Our aim was to define radiographic reference values for these parameters and to investigate potential differences related to sex and age.
Patients and methods
Retrospectively calibrated long standing anteroposterior radiographs of 254 skeletally immature patients with a chronological age ranging from 8 to 16 years were analyzed. All radiographs were obtained from the archives of University Hospital of Muenster, Germany during the past 10 years. The radiographs originated from patients treated in our outpatient department. The reasons for radiographic assessment were ruling out pathological limb alignment, follow-up of permanent or temporary unilateral (hemi-)epiphysiodesis of the distal femur or the proximal tibia for LLD or angular deformities, and the overall assessment of LLD. Only non-affected, healthy, and untreated legs were analyzed. The same patient cohort had already been used previously to establish standard radiographic reference values for proximal fibular height in growing patients [18]. The following inclusion criteria were defined: chronological patient age 8–16 years, open distal femoral and proximal tibial growth plate, LLD < 1 cm, MAD < ±2 cm. Both lower limbs of patients who underwent operative treatment of the knee joint, who received systemic treatment like chemotherapy or growth hormone medication or with evidence of maltorsion, congenital disorders, congenital limb deficiency, or history of trauma were excluded from the study. Radiographs with technical deficiencies such as malorientation of the legs during examination or inaccurate stitching were also excluded from analysis. Whenever both legs from one patient met the inclusion criteria bilateral measurements were conducted. This led to radiological assessment of 445 legs in the femoral group, 204 females (f) and 241 males (m) legs, and 497 legs in the tibial group, 228 (f) and 269 (m) legs.
Radiographic technique and measurement parameters
Long standing radiographs were captured from a defined distance of 2.8 meters with a metal calibration sphere of 25.4 mm diameter. If present, LLD was equalized by blocks under the shortened leg until the pelvis reached level position and adequate orientation was assured by pointing the patellae forward. The long standing radiographs were fused digitally, stitching 3–4 sector radiographs together.
4 radiographic parameters were assessed: (1) femoral floor angle, (2) tibial roof angle, (3) width at femoral physis, and (4) femoral notch–intercondylar distance (Figure). The values were measured in different age groups (Table 1). These radiographic measurements have partially been used in previous studies [13-15]. However, their physiological ranges have never been validated.
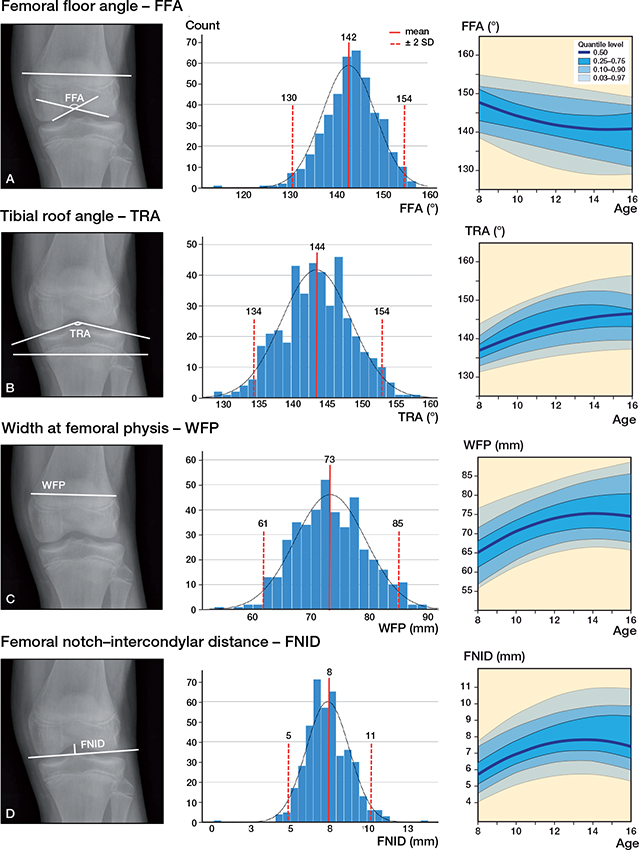
Left panels: anteroposterior long standing radiograph of a 13-year-old male. (A) The femoral floor angle (FFA) is the angle facing the physis between the femoral slope lines). (B) The tibial roof angle (TRA) is the angle facing the physis between the tibial plateau lines. (C) Width at femoral physis (WFP) is the distance between the ends of the distal femoral physis. (D) Femoral notch–intercondylar distance (FNID) is the perpendicular distance between the most proximal point of the femoral notch and a line through the most distal part of the femoral condyles.
Middle panels: The histograms depict a normal distribution of the measurement values of the entire study population (age 8–16 years) with mean and ± 2 SDs.
Right panels: Development of FFA, TRA, WFP, and FNID in children aged from 8 to 16 years. The graphs were replicated with the standard percentiles used by the Centers for Disease Control (3% and 97%).
To assess inter-rater reliability using intraclass correlation coefficients (ICCs), 2 observers independently measured the femoral floor angle, femoral notch–intercondylar distance, and the width at femoral physis in 126 radiographs and the tibial roof angle in 138 radiographs, using 2-way mixed-effect models for absolute agreement. All measurements were performed on calibrated radiographs with the PACS System (GE Healthcare, Chicago, IL, USA).
Statistics
The data distribution pattern of the measurements was analyzed descriptively by using histograms. Binary variables were illustrated numerically with percentages. Normally distributed continuous variables were reported with means, standard deviations (SD), and 95% confidence intervals (CI). Median values with interquartile ranges (IQR), given as 25th percentile to 75th percentile, were calculated for non-normally distributed variables.
A linear mixed model (LMM) was used to investigate the effect of age and sex as independent variables (fixed effects) on the 4 outcome variables femoral floor angle, tibial roof angle, width at femoral physis, and femoral notch–intercondylar distance as dependent variables. To account for intraindividual correlation, a random intercept for the patient was added to the model. The model fit was assessed descriptively using Q–Q plots. An additional mixed model was computed using the age groups as single fixed effect. Effect estimates, 95% confidence limits, and P values were presented. No adjustments for multiple testing have been done.
To calculate age-dependent percentile curves, quantile regression as introduced by Koenker and Bassett [19] and Koenker and Hallock [20] was used. The quantile regression used in this study was based on least absolute deviations estimation as median regression is more robust to outliers than least squares regression. Percentile curves for the following quantiles were calculated: 0.03, 0.1, 0.25, 0.50, 0.75, 0.90, and 0.97. Analyses were conducted using the statistical analysis software SAS 9.4 (SAS Institute, Cary, NC, USA). Quantile regression analyses were performed using the procedure QUANTREG and the linear mixed models were calculated with the procedure Mixed.
For the 2 raters ICC was calculated based on the estimated variance components of a linear mixed model including a fixed effect for the rater and a random effect for each of the patient and the leg of the patient. 95% CI was computed using a parametric bootstrap (10,000 runs). Sample size calculation for 2 independent raters was performed with STATA/MP 17.0 (StataCorp LLC, College Station, TX, USA) by assessing the width of a 2-sided 95% CI for the ICC.
Ethics, data sharing, funding, and disclosures
The study was approved by the ethical committee of the University of Muenster on November 21, 2017 (registration number 2017-491-f-S). The ethical approval does not permit sharing of raw data. The authors received no funding for this work and have no conflicts of interest. Completed disclosure forms for this article following the ICMJE template are available on the article page, doi: 10.2340/17453674.2023.15336
Results
The mean age of the study cohort was 12.4 years (SD 2, CI 12.2–12.6) and normal distribution was observed for all 4 measurement parameters (Figure). The mean femoral floor angle was 142° (SD 6, CI 141.8–142.9), mean tibial roof angle was 144° (SD 5, CI 143.7–144.1), mean width at femoral physis was 73 mm (SD 6, CI 72.8–73.9), and mean femoral notch–intercondylar distance was 8 mm (SD 1, CI 7.5–7.7) (Figure, Table 2). On analyzing potential age- and sex-dependent discrepancies of the measurements we found statistically significant differences associated with age regarding the femoral floor angle, tibial roof angle, and width at femoral physis (Table 3). A sexdependent statistically significant difference was observed only for the femoral notch–intercondylar distance (Table 3).
To facilitate the clinical applicability, the quantile levels for the 4 measurements by age were graphed to illustrate the development of the angles and distances by age (Figure). The graphs were replicated with the standard percentiles according to the Centers for Disease Control and Prevention (3% and 97%) [21].
The estimated ICCs were excellent for all measurements (femoral floor angle: 0.90, CI 0.82–0.94, tibial roof angle: 0.88, CI 0.72–0.94, width at femoral physis: 0.98, CI 0.98–0.99, femoral notch–intercondylar distance: 0.93, CI 0.43–0.98) (Table 4).
Discussion
We aimed to define radiographic reference values for the central knee anatomy of 8–16-year-old children and to investigate potential differences related to sex and age. The Figure provides an overview of the physiological range of the evaluated femoral floor angle, tibial roof angle, width at femoral physis, and femoral notch–intercondylar distance.
Our results are important as previous studies have assessed the potential risk of iatrogenic angular deformities of epiphysiodesis around the knee for correction of LLD or hemi-epiphysiodesis of the distal femur or proximal tibia for correction of angular deformities [5,9,22-25]. Less attention has been given to potential treatment-associated alterations of the central knee joint anatomy in the coronal plane. 3 studies have tried to analyze potential changes in the intra-articular knee anatomy during (hemi-)epiphysiodesis [13-15]. Sinha et al. analyzed 42 children who either underwent temporary hemi-epiphysiodesis of the proximal tibia for correction of angular deformities (n = 34) or temporary medial and lateral epiphysiodesis for treatment of LLD (n = 8) with tension band plates. They reported a decrease of the tibial roof angle by a mean of 5° in their patient cohort and concluded that the osseous morphology of the tibial plateau changed compared with the non-operated side in a significant number of patients [14]. Tolk et al. retrospectively evaluated 34 patients treated for LLD by means of epiphysiodesis around the knee with tension band plates (distal femur n = 24, proximal tibia n = 6, distal femur and proximal tibia n = 4) [15]. In accordance with Sinha et al. regarding the tibial roof angle they reported a statistically significant difference between the operated and the nonoperated leg of 8° and a statistically significant postoperative decrease of 5° in the treated leg. They also found a statistically non-significant change of the femoral floor angle [15]. Ballhause et al. retrospectively analyzed 44 patients who were treated by temporary hemi-epiphysiodesis of the proximal tibia with tension band plates due to angular deformities. Just like Sinha et al. and Tolk et al. the authors measured the tibial roof angle of the treated knee and compared it with mean values of 25 untreated knees [13]. In contrast to the 2 aforementioned studies, Ballhause et al. could not confirm statistically significant changes of the tibial roof angle [13]. However, due to the lack of standardized reference values regarding the central knee anatomy in growing patients, neither Sinha et al., Tolk et al., nor Ballhause et al. were able to interpret whether the observed alterations in the central knee anatomy remained within physiological margins [13-15]. Given the absence of assessment in the literature, it is challenging to interpret the parameters’ width at femoral physis and femoral notch–intercondylar distance in relation to potential treatment-related alterations among patients undergoing (hemi-)epiphysiodesis of the distal femur and proximal tibia. However, both parameters have been employed by studies outside the field of growth-modulating treatment [26-31]. Width at femoral physis has been used as a descriptive parameter for femoral morphology in children or quantitatively to assess skeletal age [28,29] but clinical consequences of potential alterations remain to be described. One could assume that an uneven distribution of growth arrest could influence this parameter. Several other studies have assessed the relationship between the femoral notch–intercondylar distance and stability of the anterior cruciate ligament [26,27,30-32]. Iriuchishima et al. observed a higher incidence of anterior cruciate ligament injury in patients with a relatively short femoral notch–intercondylar distance [31]. Flattening of the femoral notch measured as decreased femoral notch–intercondylar distance in patients who underwent epiphysiodesis of the medial and lateral femur has been described [15]. If and how this observation affects the stability of the anterior cruciate ligament has not yet been evaluated.
We found that the femoral floor angle, tibial roof angle, width at femoral physis, and femoral notch–intercondylar distance are normally distributed parameters in children aged 8–16 years (Figure). We propose that values within 2 SD be considered as physiological. Statistically significant age-dependent changes were observed for the femoral floor angle, tibial roof angle, and width at femoral physis, and a sex-dependent statistically significant difference was observed for the femoral notch–intercondylar distance. However, the few changes that were statistically significant all remained within the margins of 2 SD, and we caution the reader not to overinterpret the observed statistically significant differences, which are most likely without clinical relevance. It is unlikely that the complex anatomy of the knee joint is clinically affected by isolated alterations of the aforementioned radiographic parameters in the coronal plane if they remain within the margin of 2 SD. One hypothetical explanation for the observed sex-dependent statistically significant change regarding the femoral notch–intercondylar distance could be that in general the overall size of the femur in males is slightly bigger than in girls.
Taking the radiographic reference values of our study into consideration, the variations in the tibial roof and femoral floor angle reported in the studies of Sinha et al., Tolk et al., and Ballhause et al. all remained within physiological margins [13-15]. Contrary to the conclusion of Sinha et al. and Tolk et al. this might indicate that growth-modulating treatment such as temporary epiphysiodesis around the knee or hemi-epiphysiodesis of the proximal tibia may rarely lead to pathological central knee anatomy. Extreme changes in one individual from one end of the described physiological ranges to the other could possibly have a clinical impact but require further investigation regardless.
Limitations
This study has several limitations. First, this is a retrospective radiographic analysis, which does not provide information on how much change in central knee anatomy could be clinically relevant. All measurements were conducted on calibrated long standing anteroposterior radiographs and thus different techniques of radiographic analysis, i.e., positioning of the patella and stitching techniques, might lead to variations in the assessed parameters. Therefore, the suggested reference values can only be applied for long standing anteroposterior radiographs. In addition, varying patient posture during radiographic examination might also provoke measurement inaccuracies. Furthermore, one might consider that 2-dimensional radiographs might not be sufficient to assess the complex 3-dimensional anatomy of the knee joint. However, long standing anteroposterior radiographs under full weight-bearing remain the gold standard when planning deformity correction of the lower limb. This study is only a combined radiographic and statistical approach to assess the physiological range of 4 measurement parameters of the central knee in the coronal plane. Conclusions regarding long-term effects or clinical aspects such as knee instability or pain cannot be drawn.
Conclusion
This study provides new radiographic reference values of the central knee anatomy in the coronal plane for children between 8 and 16 years of age.
In perspective, considering the reference values for the femoral floor and tibial roof angle presented in this study, it seems likely that previously reported changes of the central knee anatomy related to (hemi-)epiphysiodesis of the distal femur and proximal tibial all remained within physiological margins. Based on these reference values future studies should investigate if and how central knee anatomy is altered by growth modulation treatment around the knee.
- Vogt B, Roedl R, Gosheger G, Frommer A, Laufer A, Kleine-Koenig M T, et al. Growth arrest: leg length correction through temporary epiphysiodesis with a novel rigid staple (RigidTack). Bone Joint J 2021; 103-b: 1428-37. doi: 10.1302/0301-620X.103B8.BJJ-2020-1035.R4.
- Canale S T, Christian C A. Techniques for epiphysiodesis about the knee. Clin Orthop Relat Res 1990; (255): 81-5.
- Raab P, Wild A, Seller K, Krauspe R. Correction of length discrepancies and angular deformities of the leg by Blount’s epiphyseal stapling. Eur J Pediatr 2001; 160: 668-74. doi: 10.1007/s004310100834.
- Ghanem I, Karam J A, Widmann R F. Surgical epiphysiodesis indications and techniques: update. Curr Opin Pediatr 2011; 23: 53-9. doi: 10.1097/MOP.0b013e32834231b3.
- Stevens P M. Guided growth for angular correction: a preliminary series using a tension band plate. J Pediatr Orthop 2007; 27: 253-9. doi: 10.1097/BPO.0b013e31803433a1.
- Vogt B, Toporowski G, Gosheger G, Laufer A, Frommer A, Kleine-Koenig M T, et al. Guided growth: angular deformity correction through temporary hemiepiphysiodesis with a novel flexible staple (FlexTack). Bone Joint J 2023; 105-B: 331-40. doi: 10.1302/0301-620X.105B3.BJJ-2022-0857.R1.
- Phemister D B. Operative arrestment of longitudinal growth of bones in the treatment of deformities. J Bone Joint Surg Am 1933; 15.
- Blount W P, Clarke G R. Control of bone growth by epiphyseal stapling: a preliminary report. J Bone Joint Surg Am 1949; 31(3): 464-78.
- Metaizeau J P, Wong-Chung J, Bertrand H, Pasquier P. Percutaneous epiphysiodesis using transphyseal screws (PETS). J Pediatr Orthop 1998; 18: 363-9.
- Vogt B, Frommer A, Gosheger G, Toporowski G, Tretow H, Rödl R, et al. [Growth modulation through hemiepiphysiodesis: novel surgical techniques: risks and progress]. Orthopade 2021; 50: 538-47. doi: 10.1007/s00132-021-04122-8.
- Stevens P, Desperes M, McClure P K, Presson A, Herrick J. Growth deceleration for limb length discrepancy: tension band plates followed to maturity. Strategies Trauma Limb Reconstr 2022; 17: 26-31. doi: 10.5005/jp-journals-10080-1548.
- Braga S R, Santili C, Rodrigues N V M, Soni J F, Green D W. Growth modulation for angular knee deformities: a practical guideline. Curr Opin Pediatr 2023; 35(1): 110-17. doi: 10.1097/mop.0000000000001183.
- Ballhause T M, Stiel N, Breyer S, Stücker R, Spiro A S. Does eight-plate epiphysiodesis of the proximal tibia in treating angular deformity create intra-articular deformity? Bone Joint J 2020; 102-b: 14128. doi: 10.1302/0301-620X.102B10.BJJ-2020-0473.R1.
- Sinha R, Weigl D, Mercado E, Becker T, Kedem P, Bar-On E. Eight-plate epiphysiodesis: are we creating an intra-articular deformity? Bone Joint J 2018; 100-b: 1112-16. doi: 10.1302/0301-620X.100B8.BJJ-2017-1206.R3.
- Tolk J J, Merchant R, Calder P R, Hashemi-Nejad A, Eastwood D M. Tension-band plating for leg-length discrepancy correction. Strategies Trauma Limb Reconstr 2022; 17: 19-25. doi: 10.5005/jp-journals-10080-1547.
- Moreland J R, Bassett L W, Hanker G J. Radiographic analysis of the axial alignment of the lower extremity. J Bone Joint Surg Am 1987; 69: 745-9.
- Paley D. Principles of deformity correction. 1st ed. Berlin: Springer; 2002. doi: 10.1007/978-3-642-59373-4.
- Frommer A, Niemann M, Gosheger G, Toporowski G, Laufer A, Eveslage M, et al. A new standard radiographic reference for proximal fibular height in children. Acta Orthop 2020; 91: 611-16. doi: 10.1080/17453674.2020.1769378.
- Koenker R, Bassett G. Regression quantiles. Econometrica 1978; 46: 33-50.
- Koenker R, Hallock K F. Quantile regression. J Economic Perspectives 2001; 15: 143-56.
- Centers for Disease Control and Prevention, National Center for Health Statistics: Growth Charts. Atlanta, GA: CDC; 2010.
- Pendleton A M, Stevens P M, Hung M. Guided growth for the treatment of moderate leg-length discrepancy. Orthopedics 2013; 36: e575-e580. doi: 10.3928/01477447-20130426-18.
- Frommer A, Niemann M, Gosheger G, Eveslage M, Toporowski G, Laufer A. Temporary proximal tibial epiphysiodesis for correction of leg length discrepancy in children: should proximal fibular epiphysiodesis be performed concomitantly? J Clin Med 2021;10(6): 1245. doi: 10.3390/jcm10061245.
- Laufer A, Toporowski G, Gosheger G, von der Heiden A, Rölfing J D, Frommer A, et al. Preliminary results of two novel devices for epiphysiodesis in the reduction of excessive predicted final height in tall stature. J Orthop Traumatol 2022; 23: 46. doi: 10.1186/s10195-022-00666-3.
- Gorman T M, Vanderwerff R, Pond M, MacWilliams B, Santora S D. Mechanical axis following staple epiphysiodesis for limb-length inequality. J Bone Joint Surg Am 2009; 91: 2430-9. doi: 10.2106/JBJS.H.00896.
- Liu R W, Farrow L D, Messerschmitt P J, Gilmore A, Goodfellow D B, Cooperman D R. An anatomical study of the pediatric intercondylar notch. J Pediatr Orthop 2008; 28: 177-83. doi: 10.1097/BPO.0b013e318165219b.
- Lima F M, Debieux P, Aihara A Y, Cardoso F N, Franciozi C E, Grimberg A, et al. The development of the intercondylar notch in the pediatric population. Knee 2020; 27: 747-54. doi: 10.1016/j.knee.2020.04.020.
- Bertocci G, Brown N P, Thompson A, Bertocci K, Adolphi N L, Dvorscak L, et al. Femur morphology in healthy infants and young children. Clin Anat 2022; 35: 305-15. doi: 10.1002/ca.23825.
- Knapik D M, Sanders J O, Gilmore A, Weber D R, Cooperman D R, Liu R W. A quantitative method for the radiological assessment of skeletal maturity using the distal femur. Bone Joint J 2018; 100-b: 1106-11. doi: 10.1302/0301-620X.100B8.BJJ-2017-1489.R1.
- Iriuchishima T, Goto B, Fu F H. The radiographic tibial spine area is correlated with the occurrence of ACL injury. Knee Surg Sports Traumatol Arthrosc 2022; 30: 78-83. doi: 10.1007/s00167-021-06523-w.
- Iriuchishima T, Goto B, Fu F H. The occurrence of ACL injury influenced by the variance in width between the tibial spine and the femoral intercondylar notch. Knee Surg Sports Traumatol Arthrosc 2020; 28: 3625-30. doi: 10.1007/s00167-020-05965-y.
- Farrow L D, Chen M R, Cooperman D R, Victoroff B N, Goodfellow D B. Morphology of the femoral intercondylar notch. J Bone Joint Surg Am 2007; 89: 2150-5. doi: 10.2106/JBJS.F.01191.
- Vogt B, Schiedel F, Rödl R. [Guided growth in children and adolescents: correction of leg length discrepancies and leg axis deformities]. Orthopade 2014; 43: 267-84. doi: 10.1007/s00132-014-2270-x.