Complications after lateral unicompartmental knee arthroplasty in a fast-track setting: a prospective cohort study of 170 procedures
Kristine I BUNYOZ 1, Christoffer Calov JØRGENSEN 2, Pelle Baggesgaard PETERSEN 2, Henrik KEHLET 2, Kirill GROMOV 1, and Anders TROELSEN 1; on behalf of the Lundbeck Foundations Centre for Fast-track Hip and Knee Replacement Collaborative Group a
1 Department of Orthopaedic Surgery, Clinical Orthopaedic Research Hvidovre (CORH), Copenhagen University Hospital Hvidovre; 2 Section for Surgical Pathophysiology, Rigshospitalet, Copenhagen University Hospital, Denmark
a The Centre for Fast-track Hip and Knee Replacement Collaborative Group: Frank MADSEN, Department of Orthopedics, Aarhus University Hospital, Aarhus, Denmark; Torben Bæk HANSEN, Department of Orthopedics, Regional Hospital Holstebro and University of Aarhus, Holstebro, Denmark; Mogens LAURSEN, Aalborg University Hospital Northern Orthopaedic Division, Aalborg, Denmark; Lars Tambour HANSEN, Department of Orthopedics, Sydvestjysk Hospital Esbjerg/Grindsted, Grindsted, Denmark; Claus VARNUM, Department of Orthopedics, Vejle Hospital, Vejle, Denmark; Mikkel Rathsach ANDERSEN, Department of Orthopedics, Gentofte University Hospital, Copenhagen, Denmark; Niels Harry KRARUP, Department of Orthopedics, Viborg Hospital, Viborg, Denmark; and Henrik PALM, Department of Orthopaedic Surgery, Copenhagen University Hospital Bispebjerg, Copenhagen, NV, Denmark
Background and purpose — In existing studies on fasttrack unicompartmental knee arthroplasty (UKA), the majority of surgeries are medial. There are substantial differences between lateral and medial UKA, which is why outcomes cannot automatically be compared. To gain information on the feasibility and safety of fast-track protocols in lateral UKAs, we investigated length of stay (LOS) and early complications after lateral UKA, performed using a fast-track protocol in well-established fast-track centers.
Patients and methods — We retrospectively evaluated prospectively collected data on patients undergoing lateral UKA in a fast-track setup from 2010 to 2018 at 7 Danish fast-track centers. Data on patient characteristics, LOS, complications, reoperations, and revisions was analyzed using descriptive statistics. Safety and feasibility were defined as complication and reoperation rates within 90 days comparable to non-fast track lateral UKA or fast-track medial UKA.
Results — We included 170 of patients with a mean age of 66 (SD 12) years. Median LOS was 1 day (interquartile range 1–1), which was unchanged from 2012–2018. 18% were discharged on the day of surgery. Within 90 days, 7 patients experienced medical complications and 5 patients experienced surgical complications. 3 patients underwent reoperation, 2 were soft tissue revisions and the third was removal of an exostosis due to catching of the patella. 1 patient was revised due to a bearing dislocation.
Conclusion — Our findings suggest that lateral UKA in a fast-track setting is feasible and safe.
Citation: Acta Orthopaedica 2023; 94: 316–320. DOI: https://doi.org/10.2340/17453674.2023.13653.
Copyright: © 2023 The Author(s). This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (https://creativecommons.org/licenses/by-nc/4.0/), allowing third parties to copy and redistribute the material in any medium or format and to remix, transform, and build upon the material for non-commercial purposes, provided proper attribution to the original work.
Submitted: 2022-11-03. Accepted: 2023-04-27; Published: 2023-06-27.
Correspondence: kristine.ifigenia.bunyoz@regionh.dk
AT, KG, and HK contributed to the conception of the study. PBP and CJ gathered data. KIB analyzed the data and wrote the first draft of the manuscript. All authors and collaborators revised the draft and approved the final manuscript.
The authors would like to thank the participating centers for gathering information for this study.
Handling co-editors: Keijo Mäkelä and Robin Christensen
Acta thanks Henrik Bodén, Tuukka Niinimäki, and Annette W-Dahl for help with peer review of this manuscript.
Fast-track protocols have enhanced recovery after primary and revision total knee arthroplasty (TKA), resulting in reduced length of stay (LOS), morbidity, and mortality [1-3]. Favorable safety profiles and reduction of costs have further increased the interest in these protocols [2]. Unicompartmental knee arthroplasty (UKA) patients have a shorter length of postoperative stay than TKA and fast-track protocols have proven safe and applicable in UKA [4,5].
Lateral unicompartmental tibiofemoral osteoarthritis (OA) is less frequent than medial unicompartmental tibiofemoral OA, and it projects to constitute only 5–10 % of UKAs and less than 1% of all knee arthroplasties [6,7]. As isolated lateral compartment OA is estimated in approximately 10% of OA patients [8] the procedure is potentially underutilized. Furthermore, lateral UKA is considered to be technically more demanding than medial UKA due to the functional anatomy of the lateral compartment [9]. Consequently, the literature is sparse, mostly involving retrospective studies with a low number of included patients [10-15]. The limited number of lateral UKAs also applies to studies on enhanced recovery, where up to 96% are medial UKAs [4,16,17]. Others have not reported the share of medial and lateral UKAs in their population. Due to the substantial differences between lateral and medial knee anatomy, kinematics, and surgical technique, results from medial UKAs cannot automatically be extrapolated to lateral UKAs [9,18]. Therefore we need specific information concerning the feasibility and safety of lateral UKA using a fast-track setting. The aim of our study was to report LOS and describe complications, reoperations, and revisions after lateral UKA, when performed in 7 already well-established fast-track centers over a 9-year period.
Patients and methods
This cohort study retrospectively evaluated prospectively collected data on primary lateral UKAs reported to the Lundbeck Foundation Centre for Fast-track Hip and Knee Replacement database (LCDB) from 2010 to 2018 (end of August) [19]. The LCDB includes data from 9 dedicated orthopedic fasttrack centers across Denmark. Of these centers, 7 perform lateral UKAs. Thus, we included data on 170 lateral UKA procedures from 7 fast-track centers (Figure). As previously reported [19], the fast-track protocol includes the intention to use spinal anesthesia, multimodal opioid-sparing analgesia, high-dose preoperative corticosteroids, preoperative intravenous tranexamic acid, no drains, early mobilization (< 6 hours) with full weight-bearing, and discharge to the patient’s own home based on a set of functional discharge criteria. Inhospital only thromboprophylaxis was administrated in cases with LOS < 5 days. For lateral UKA the prevailing approach is to use a tourniquet, but the decision was left to the preference of the surgeon. Data on comorbidities was collected using preoperative nurse-assisted patient-reported questionnaires [19]. Indication for surgery, LOS, and readmissions within 90 days were acquired from the Danish National Patient Registry (DNPR) resulting in > 99% completion [20]. Information regarding prescribed potent anticoagulants, diabetic treatment, and psychotropic medication was obtained from the Danish National Database of Reimbursed Prescriptions (DNDRP). The LOS was defined as the number of nights spent in hospital. Complications were divided into medical and surgical complications [19]. Only complications and readmissions with a potential relation to the performed arthroplasty were included in the analysis. This included readmissions with not already known medical conditions, readmissions with relation to the wound (e.g., infection, wound healing problems, hematomas), readmissions due to not obtaining adequate mobilization, and readmissions due to reoperations or revisions related to the lateral UKA. A reoperation was defined as any surgery requiring anesthesia, performed without the removal or replacement of a prosthetic component. A revision was defined as any surgery with the removal, addition, or replacement of a prosthetic component. Evaluation of safety and feasibility were based on complication and reoperation rates within 90 days comparable to non-fast track lateral UKA or fast-track medial UKA.
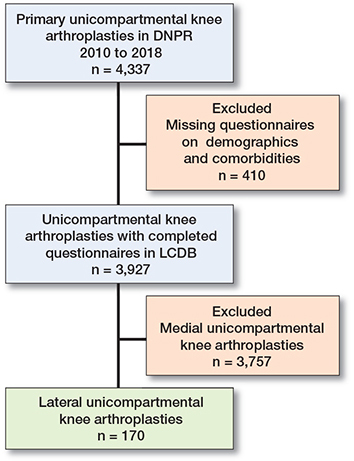
Flowchart of inclusion. DNPR = Danish National Patient Registry; LCDB = Lundbeck Foundation Centre for Fast-track Hip and Knee Replacement database.
This study follows the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guideline.
Statistics
All patients undergoing lateral UKA reported to the LCDB were included in the analysis. QQ-plots and histograms were used to determine if data was either normally distributed or skewed. Normally distributed data was reported as means (SD) and skewed data as medians (IQR). Categorical data was reported as numbers and proportions (%). Data was analyzed using RStudio version 4.2.0 (R Foundation for Statistical Computing, Vienna, Austria)
Ethics, data sharing plan, funding, and disclosures
As this study was non-interventional, no ethical approval was needed. The Danish National Board of Health (3-30313-56/2/EMJO) permitted data retrieval. Storing data was approved by the Danish Data Protection Agency (P2019-709). Data sharing will be available upon reasonable request to the corresponding author. This study did not receive any funding and the authors declare no conflict of interest in relation to this manuscript. Completed disclosure forms for this article following the ICMJE template are available on the article page, doi: 10.2340/17453674.2023.13653
Results
Lateral UKAs constituted 0.8% of all knee arthroplasties performed in all the centers. We included 170 lateral UKAs. Most surgeries were in males (72%) and due to primary lateral knee OA (86%). The mean age was 66 years (SD 12) and mean body mass index (BMI) was 27.4 (SD 4.1). Patient characteristics, including comorbidities and medical history of venous thromboembolism (VTE), are presented in Table 1. During the study period, the median LOS was 1 day (IQR 1–1; mean 1.2 [SD 1.1]) and number of surgeries per year varied between 11 and 33. A median LOS of 1 day was consistent from 2012 to 2018. At individual center level, a median LOS of 1 day applied in 5 of the 7 fast-track centers (Table 2). 18% (30/170) of the patients were discharged on the day of surgery and 88% (120/170) were discharged within 2 days. The number of patients discharged on the day of surgery varied between 0% and 50% in the included centers (Table 2). Within the first 90 days, there were 7 medical complications and 5 surgical complications (Table 3). Of the 5 surgical complications, 4 patients underwent reoperation. 2 of those were soft tissue revision due to wound infection and wound rupture, 1 was removal of an exostosis due to catching of the patella, and the last was an aseptic revision due to dislocation of the bearing. 1 surgical complication (the hematoma) did not require any surgical intervention. Complications and all contact with the hospital within the first 90 days are listed in Table 4 (see Appendix). 1 patient died 81 days after surgery, giving overall 90-day mortality of 0.6%. The death did not happen during hospital admission and details concerning the cause of death were not available.
Discussion
The aim of the study was to investigate LOS and 90 days complications, reoperations, and revisions after lateral UKA performed in a fast-track setting. We found a median LOS of only 1 day, which was unchanged from 2012 to 2018. 7 patients experienced a medical complication, and 5 patients experienced a surgical complication within the first 90 days after surgery.
The median LOS is similar to what was found by Gromov et al. including largely (96%) medial UKAs [4], but lower than LOS after fast-track TKA [16,21]. The study by Gromov et al. [4] and Jensen et al. [16] is based on similar fast-track protocols. The current literature on lateral UKA without enhanced recovery protocols focus on revision rates, survival, and follow-up time rather than LOS, making comparisons difficult. A median LOS of 1 day is comparable to the median LOS for all medial UKAs performed in Denmark in 2020 (median LOS 1 day), as reported by the Danish Knee Arthroplasty Register in the 2021 annual report [22]. This could imply that lateral UKAs have the same potential as medial UKAs in terms of postoperative mobilization and LOS, even though substantial differences exist between the 2 procedures.
Whether a LOS of 1 day is solely due to the fast-track protocol is uncertain, as there are no reports on LOS for lateral UKAs performed without a fast-track setting for comparison.
The number of same-day discharges was 30/170 (18%). This is lower than previous studies on unspecified UKAs in a similar fast-track setting, which report same-day discharge of 25.4% and 21.1%, respectively [4,16]. However, in a recent report by Wainwright, including data from English NHS providers, the overall day-case rate for UKA was 5.4% [23].
We experienced 12 (7%) complications (medical and surgical) that were deemed attributable to the surgical procedure, all of them resulting in readmission within the first 90 days. This is higher than a previous fast-track study on unspecified UKAs, which found a total complication rate of 5.5% [16]. Separating the medical and surgical complications, the number of medical complications in our study (7/170, 4%) was comparable to the percentage of medical complications for unspecific UKAs (3.7%) [16]. However, the number of surgical complications was slightly higher (5/170, 2.9%) than in unspecific UKAs (1.8%) [16]. This could support the opinion of lateral UKA being more technically demanding. It can be debated whether 2 of the complications (lack of mobilization, wound rupture) could have been avoided in a non-fast-track setting with longer hospital admission, which further emphasizes the importance of patient selection. On the contrary, it has previous been described that the complication rates after UKA do not increase with the use of enhanced recovery and might even portend a safer postoperative course [5,24]. Further, whether additional complications could have arisen in the absence of a fast-track protocol is unknown.
Among the surgical complications, 4 patients (2.4%) underwent further surgery (3 reoperations and 1 mechanical revision). As there are no current studies reporting on enhanced recovery and reoperations on lateral UKAs, a revision rate of 1/170 (0.6%) can therefore only be compared with short-term follow-up studies (mean follow-up 1.9–3 years) on isolated lateral UKA, which have reported revision rates between 0% and 3.3% [14,25,26].
In our study, we were not able to determine whether a fixed or mobile-bearing prosthesis was used in individual cases, but we experienced 1 case of bearing dislocation in this short follow-up period. We know that one of the included centers used a mobile-bearing lateral UKA prosthesis for a short period of time. The rest of the centers used a fixed-bearing prosthesis during the whole study period. In the past mobile-bearing lateral UKAs have presented unacceptable dislocation rates, thus many favor the use of fixed-bearing prosthesis for lateral UKA [27,28]. In our study, the majority of patients receiving a lateral UKA were males, which is different from most studies that primarily report a majority of women for this procedure [14,25]. This suggests selection bias in the cohort. The less frequent utilization of lateral UKA may lead to a less uniform approach to the indications and thus selection of patients for the procedure. Most centers may still have a too restrictive approach to the utilization of lateral UKA. This is further supported by the fact that lateral UKAs constituted only 0.8% of all knee arthroplasties performed in the included centers. This number is low given the number of potential patients with isolated lateral OA described in the literature [8] and the published results on lateral UKA [6,15,25,29].
Our study has limitations. There might exist some selection bias due to surgeon preference [2], patient selection, post-operative mobilization regimes, and physiotherapist resources on the day of surgery. Furthermore, the fast-track protocol might have changed a little from 2010 to 2018. In addition, this study is a cohort study investigating only lateral UKA, without direct comparison with either medial UKA or TKA performed in the same fast-track centers.
In conclusion, we found a median LOS of 1 day and an early revision rate of 0.6% using an enhanced recovery setting. These findings suggest that fast-track lateral UKA is both feasible and safe. In addition, it seems that lateral UKA has the potential to share the same benefits and safety profile as seen for medial UKA when performed in a dedicated fast-track setting.
- Kehlet H. Fast-track hip and knee arthroplasty. Lancet 2013; 381(9878): 1600-2. doi: 10.1016/S0140-6736(13)61003-X.
- Price A J, Alvand A, Troelsen A, Katz J N, Hooper G, Gray A, et al. Knee replacement. Lancet 2018; 392(10158): 1672-82. doi: 10.1016/S0140-6736(18)32344-4.
- Savaridas T, Serrano-Pedraza I, Khan S K, Martin K, Malviya A, Reed M R. Reduced medium-term mortality following primary total hip and knee arthroplasty with an enhanced recovery program. Acta Orthop 2013; 84(1): 40-3. doi: 10.3109/17453674.2013.771298.
- Gromov K, Petersen P B, Jørgensen C C, Troelsen A, Kehlet H. Unicompartmental knee arthroplasty undertaken using a fast-track protocol. Bone Joint J 2020; 102-B(9): 1167-75. doi: 10.1302/0301-620X.102B9.BJJ-2020-0247.R1.
- Gruskay J, Richardson S, Schairer W, Kahlenberg C, Steinhaus M, Rauck R, et al. Incidence and safety profile of outpatient unicompartmental knee arthroplasty. Knee 2019; 26(3): 708-13. doi: 10.1016/J.KNEE.2019.02.002.
- Baker P N, Jameson S S, Deehan D J, Gregg P J, Porter M, Tucker K. Mid-term equivalent survival of medial and lateral unicondylar knee replacement: an analysis of data from a National Joint Registry. J Bone Joint Surg Br 2012; 94(12): 1641-8. doi: 10.1302/0301-620X.94B12.29416.
- Scott R D. Lateral unicompartmental replacement: a road less traveled. Orthopedics 2005; 28(9): 983-4. doi: 10.3928/0147-7447-20050901-34.
- Wise B L, Niu J, Yang M, Lane N E, Harvey W, Felson D T, et al. Patterns of compartment involvement in tibiofemoral osteoarthritis in men and women and in whites and African Americans. Arthritis Care Res (Hoboken) 2012; 64(6): 847-52. doi: 10.1002/ACR.21606.
- Scott C E H, Nutton R W, Biant L C. Lateral compartment osteoarthritis of the knee: Biomechanics and surgical management of end-stage disease. Bone Joint J 2013; 95-B(4): 436-44. doi: 10.1302/0301-620X.95B4.30536.
- Citak M, Cross M B, Gehrke T, Dersch K, Kendoff D. Modes of failure and revision of failed lateral unicompartmental knee arthroplasties. Knee 2015; 22(4): 338-40. doi: 10.1016/J.KNEE.2015.03.008.
- Newman S D S, Altuntas A, Alsop H, Cobb J P. Up to 10 year follow-up of the Oxford Domed Lateral Partial Knee Replacement from an independent centre. Knee 2017; 24(6): 14.21. doi: 10.1016/J.KNEE.2017.05.001.
- Walker T, Zahn N, Bruckner T, Streit M R, Mohr G, Aldinger P R, et al. Mid-term results of lateral unicondylar mobile bearing knee arthroplasty: a multicentre study of 363 cases. Bone Joint J 2018; 100-B(1): 42-9. doi: 10.1302/0301-620X.100B1.BJJ-2017-0600.R1.
- Edmiston T A, Manista G C, Courtney P M, Sporer S M, Della Valle C J, Levine B R. Clinical outcomes and survivorship of lateral unicompartmental knee arthroplasty: does surgical approach matter? J Arthroplasty 2018; 33(2): 362-5. doi: 10.1016/J.ARTH.2017.09.009.
- Walker T, Hariri M, Eckert J, Panzram B, Reiner T, Merle C, et al. Minimally invasive lateral unicompartmental knee replacement: early results from an independent center using the Oxford fixed lateral prosthesis. Knee 2020; 27(1): 235-41. doi: 10.1016/J.KNEE.2019.09.018.
- Deroche E, Batailler C, Lording T, Neyret P, Servien E, Lustig S. High survival rate and very low wear of lateral unicompartmental arthroplasty at long term: a case series of 54 cases at a mean follow-up of 17 years. J Arthroplasty 2019; 34(6): 1097-104. doi: 10.1016/J.ARTH.2019.01.053.
- Jensen C B, Petersen P B, Jørgensen C C, Kehlet H, Troelsen A, Gromov K. Length of stay and 90-day readmission/complication rates in unicompartmental versus total knee arthroplasty: a propensity-score-matched study of 10,494 procedures performed in a fast-track setup. J Bone Joint Surg Am 2021; 103(12): 1063-71. doi: 10.2106/JBJS.20.01287.
- Cross M B, Berger R. Feasibility and safety of performing outpatient unicompartmental knee arthroplasty. Int Orthop 2014; 38(2): 443-7. doi: 10.1007/S00264-013-2214-9.
- van der List J P, McDonald L S, Pearle A D. Systematic review of medial versus lateral survivorship in unicompartmental knee arthroplasty. Knee 2015; 22(6): 454-60. doi: 10.1016/J.KNEE.2015.09.011.
- Jørgensen C C, Kehlet H. Role of patient characteristics for fast-track hip and knee arthroplasty. Br J Anaesth 2013; 110(6): 972-80. doi: 10.1093/BJA/AES505.
- Schmidt M, Schmidt S A J, Sandegaard J L, Ehrenstein V, Pedersen L, Sørensen H T. The Danish National Patient Registry: a review of content, data quality, and research potential. Clin Epidemiol 2015; 7 449-90. doi: 10.2147/CLEP.S91125.
- Wei B, Tang C, Li X, Lin R, Han L, Zheng S, et al. Enhanced recovery after surgery protocols in total knee arthroplasty via midvastus approach: a randomized controlled trial. BMC Musculoskelet Disord 2021; 22(1): 856. doi: 10.1186/S12891-021-04731-6.
- Dansk Knaealloplastikregister Årsrapport. ADD SOURCE (WEB-LINK)
- Wainwright T W. The current status of daycase hip and knee arthroplasty within the English National Health Service: a retrospective analysis of hospital episode statistics data. Ann R Coll Surg Engl 2021; 103(5): 324-31. doi: 10.1308/RCSANN.2020.7142.
- Bovonratwet P, Ondeck N T, Tyagi V, Nelson S J, Rubin L E, Grauer J N. Outpatient and inpatient unicompartmental knee arthroplasty procedures have similar short-term complication profiles. J. Arthroplasty 2017; 32(10): 2935-40. doi: 10.1016/J.ARTH.2017.05.018.
- Asadollahi S, Wilson H A, Thomson F R, Vaz K, Middleton R, Jenkins C, et al. Early results of fixed-bearing unicompartmental knee replacement designed for the lateral compartment. J Orthop Surg Res 2022; 17(1): 146. doi: 10.1186/S13018-021-02896-3.
- Kim K T, Lee S, Kim J, Kim J W, Kang M S. Clinical results of lateral unicompartmental knee arthroplasty: minimum 2-year follow-up. Clin Orthop Surg 2016; 8(4): 386-92. doi: 10.4055/CIOS.2016.8.4.386.
- Ernstbrunner L, Imam M A, Andronic O, Perz T, Wieser K, Fucentese S F. Lateral unicompartmental knee replacement: a systematic review of reasons for failure. Int Orthop 2018; 42(8): 1827-33. doi: 10.1007/S00264-017-3662-4.
- Ollivier M, Abdel M P, Parratte S, Argenson J N. Lateral unicondylar knee arthroplasty (UKA): contemporary indications, surgical technique, and results. Int Orthop 2014; 38(2): 449-55. doi: 10.1007/S00264-013-2222-9.
- Deroche E, Martres S, Ollivier M, Gadeyne S, Wein F, Gunepin F X, et al. Excellent outcomes for lateral unicompartmental knee arthroplasty: Multicenter 268-case series at 5 to 23 years’ follow-up. Orthop Traumatol Surg Res 2020; 106(5): 907-13. doi: 10.1016/J.OTSR.2020.03.019.